Methicillin-resistant Staphylococcus aureus (MRSA)
The Gram-positive bacteria Staphylococcus aureus was first discovered by Scottish surgeon Sir Alexander Ogston in his garden shed “laboratory” in 1881 (the short Wikipedia article on his discovery of S. aureus makes for quite interesting reading). It is a human commensal and an opportunistic pathogen, colonizing approximately a third of all humans, particularly those with certain conditions such as HIV infection, diabetes mellitus or dialysis-dependent renal failure. Methicillin-resistant S. aureus (MRSA) are a subset of these bacteria that have become resistant to the beta-lactam class of antibiotics (which includes penicillins, cephalosporins, carbapenems), which are probably the most commonly prescribed antibiotics worldwide. Methicillin was developed by the Beecham Group (a British pharmaceutical group that has since been incorporated into GlaxoSmithKline) in 1959 to treat infections caused by penicillin-resistant S. aureus, but is no longer in production, although the name remains attached to this particular resistant bacterium.
MRSA was first described in 1961 in Surrey, UK, 2 years after the development of methicillin. Unlike the Gram-negative bacteria, whose resistance to beta-lactam antibiotics tends to be primarily due to enzymatic degradation or inactivation, S. aureus becomes resistant to beta-lactams after the acquisition of a mobile genetic element (SCCmec) that contains a gene that encodes a special cell wall building block (penicillin-binding protein 2a or PBP2a) with poor affinity for beta-lactam antibiotics. As a point of interest, not all clones of S. aureus can become MRSA (an imperfect analogy being not all of us can become successful professional tennis players, no matter how much coaching we get) – the mobile genetic element SCCmec, of which there are several iterations, being actually a foreign genetic construct that comes from other types of staphylococci.
A relatively small number of pandemic clones of MRSA then spread worldwide to other hospitals in the 1970s and 1980s, with the Hungarian clone being the major clone that was brought to Singaporean hospitals during this initial period of global spread. Since then, other successful clones of MRSA have arisen, including UK-EMRSA-15 (the “E” stands for “epidemic” – this being the 15th epidemic clone of MRSA identified in UK) that is also prevalent in all Singaporean hospitals, having probably arrived in the early part of the previous decade. MRSA has also successfully “escaped” from the hospitals, with the earliest cases of community-associated MRSA (CA-MRSA) described in the early 1990s (much to the disbelief of then “experts” of MRSA), to current endemic CA-MRSA carriage in the community in many countries, including the US, Australia and Taiwan. An excellent summary of CA-MRSA was published in the Lancet in 2010. Outbreaks of CA-MRSA have also been described in Singapore – one recent example being from a local international school. A somewhat dated timeline of MRSA in Singapore is shown below. Note that although only 2 hospitals are listed on this timeline, MRSA is found in all Singaporean hospitals.
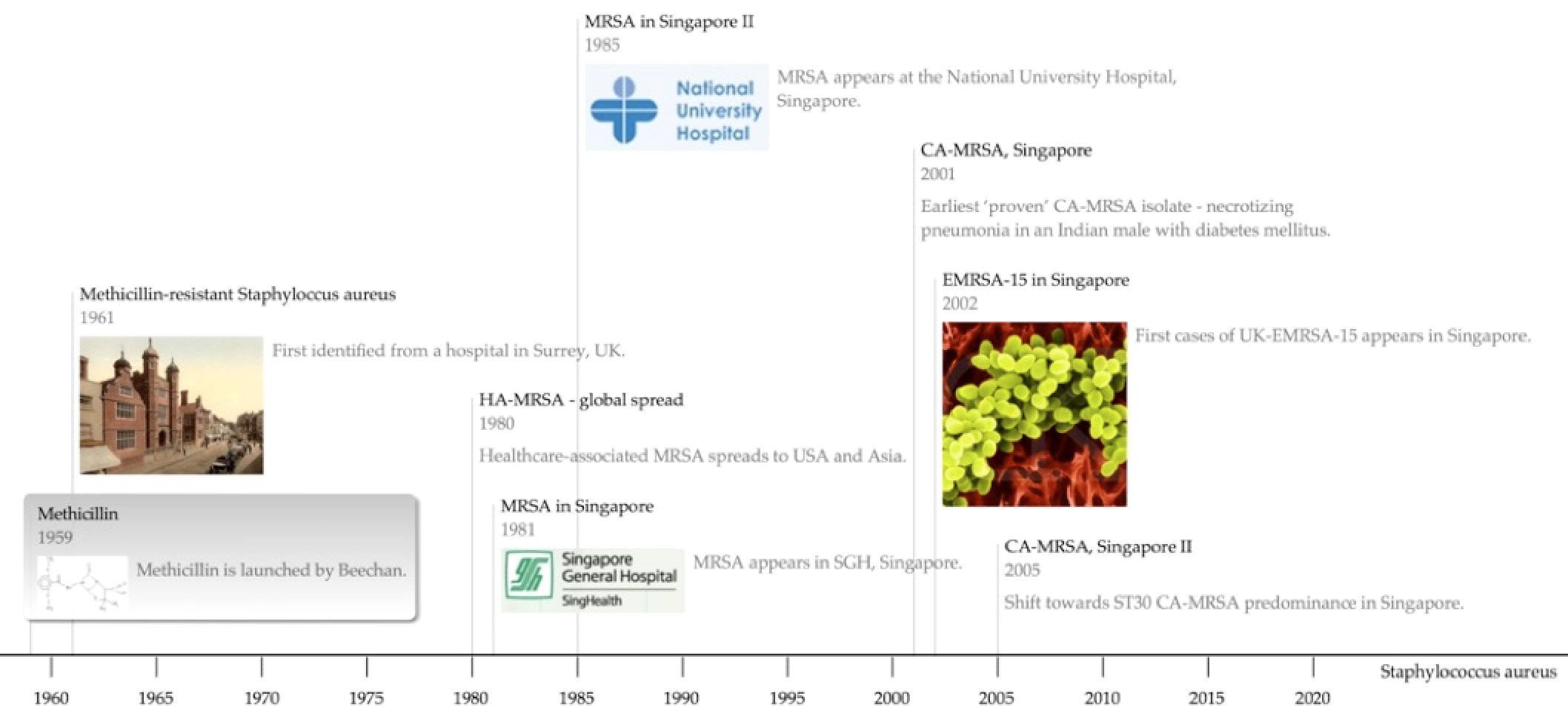
MRSA timeline, Singapore
More interestingly, MRSA has also been recently described in companion and farm animals. Some of these strains are likely passed to the animals by their human “companions”, but other clones appear to have arisen separately in the animals themselves, particularly in pigs, and may cause human disease. The most prevalent strain of pig MRSA – ST398 – has also been found in Singapore, in pigs used for research.
