Clinical Vignette 9
A middle-aged (60-year-old) man with Type 2 diabetes mellitus and past history of tuberculosis presented with low-grade fever for 2 weeks and a 1.5 cm nodule over his left lower back (approximately L1 level). This was determined to be an abscess and creamy white pus was aspirated by his general practitioner. The Gram stain showed Gram-negative bacilli, and his chest X-ray (and a segment of the subsequent CT abdomen) is shown below.
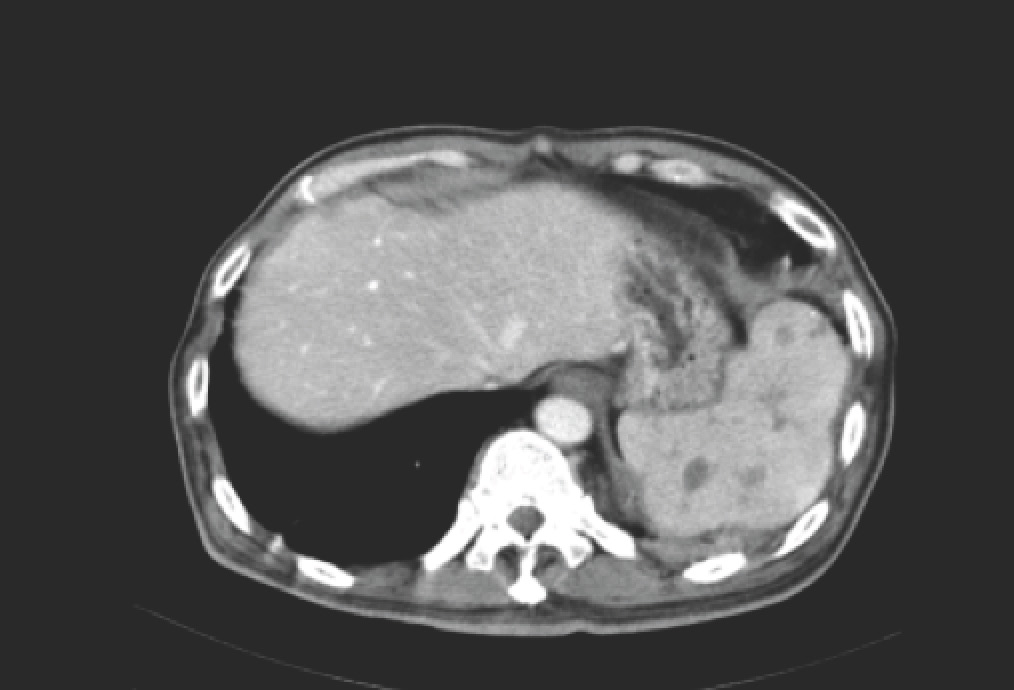
CT abdomen of the man with a nodule over his back.
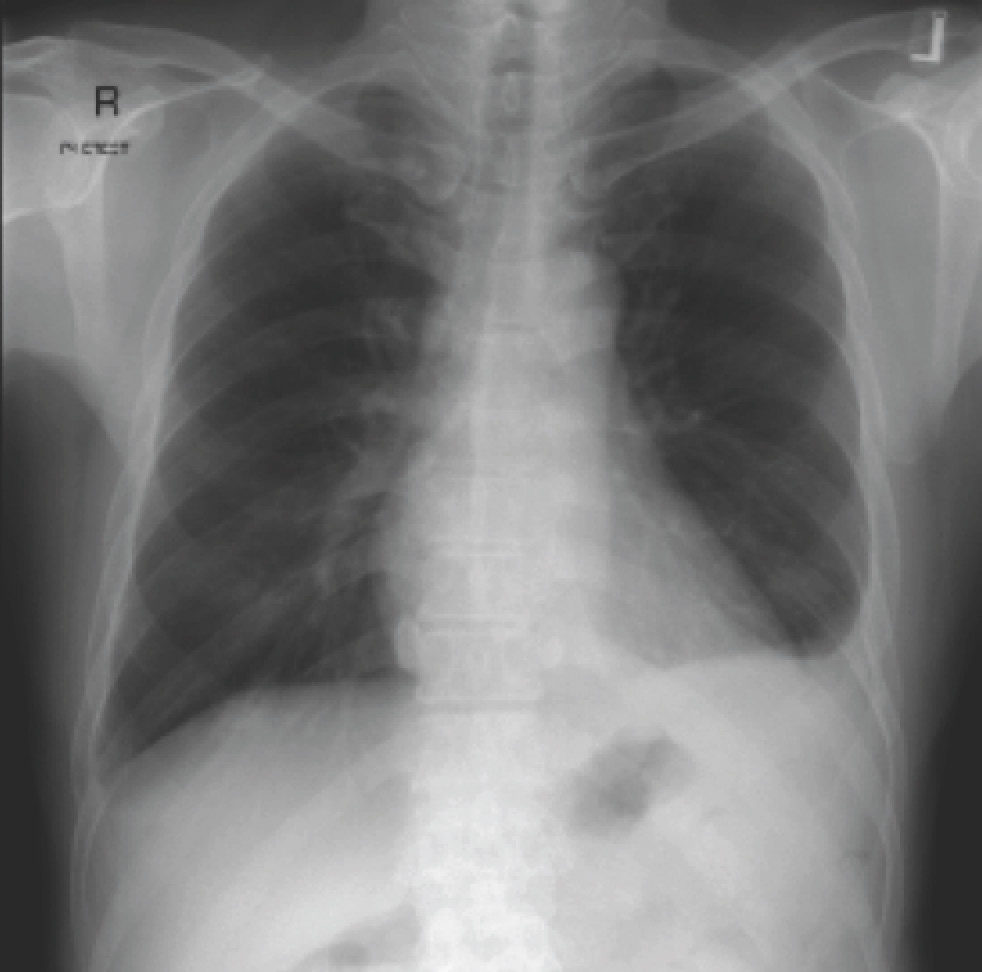
Chest X-ray of the man with a nodule over his back.
Question: What do you think is the Gram-negative bacteria isolated from the pus?
[Updated 29th November 2014]
The CT abdomen shows an irregular spleen with multiple hypodense lesions. In this context, it represents splenic abscesses. The chest X-ray shows blunting of the left costophrenic angle, representing a pleural effusion. The lower back nodule represents an abscess – in this case linked by a sinus tract to the spleen. Taking everything into consideration – Gram-negative bacteria, patient with diabetes mellitus, splenic abscesses, tropical country – the Gram-negative bacteria is almost invariably going to be Burkholderia pseudomallei, the causative agent of melioidosis. There are two key review papers – the first published in 2005 in Clinical Microbiology Reviews, and the second (behind a pay wall) published in 2012 in the New England Journal of Medicine. Current treatment protocols involve prescription of intravenous ceftazidime for 2 weeks followed by a prolonged course of oral trimethoprim/sulfamethoxazole +/- doxycycline.
