Healthcare-Associated MRSA: Singapore’s first anti-MRSA campaign (circa 1994/5)
I promised in an earlier post to discuss what I felt was the first major anti-MRSA campaign in Singapore. Although it occurred not too long ago (estimated 1994/5 – 1998/9), there are no easily obtainable records of what transpired, and I only started work right at the tail end of the “campaign” – at that time I wasn’t interested in MRSA at all! What I have managed to put together I obtained from interviews with various healthcare professionals who had been part of that initial effort, or who had “lived” through the times, or from the rare academic publications/presentations from that period. Please by all means correct the account below if you have separate knowledge of the events recounted.
Interested persons can read Prof Paul Tambyah and Dr Gamini Kumarasinghe’s account on MRSA control at the National University Hospital, Singapore, here; or go through Dr Moi Lin Ling’s presentation slides (presumably relating to the Singapore General Hospital) here.
It is probably an exaggeration to call it a “campaign”. There was no real concerted effort mounted to control MRSA in local public sector hospitals – it seemed that many of the hospitals independently started implementing similar policies around the same time, whether by word of mouth, or perceived pressure from the public or Ministry of Health Singapore (MOH). And there appeared to be an unspoken consensus to step down efforts near the start of the 21st century. While there appeared to be an infection control/MRSA guideline published by MOH in the early 1990s that was subsequently re-issued in 1998 (which meant that a national expert committee had been assembled to draft the guidelines), there was no taskforce that directed or provided oversight for all the anti-MRSA efforts in the various hospitals, nor did the hospitals share any data or lessons learned systematically. Nonetheless, these activities took place collectively around the same period of time, and therefore the label of “MRSA campaign”.
What were the policies and practices implemented at that time?
- Isolation of MRSA-infected patients. Patients who were only colonized (i.e no active infection) was exempt from isolation at most hospitals.
- Contact precautions for all MRSA-infected and -colonized patients.
- Tagging of MRSA cases (an MRSA register) so that these patients can be isolated on re-admission to the hospital. But each register was available to the frontline healthcare staff only for that particular hospital and not for other hospitals (a problem that has remained to this day in some part because of the interpretation of the Personal Data Protection Act).
- Nasal screening of MRSA-infected patients to document “clearance” of MRSA (this is because the front part of the nose, or anterior nares, is the natural “home” of Staphylococcus aureus in those of us who are colonised by this bug).
- Focus on improving hand hygiene compliance (i.e. trying to make doctors and nurses wash their hands before and after any patient contact).
Sometime during this period of time (1994-1999), the nursing homes and community hospitals – probably independently – imposed strict criteria on the transfer of patients from acute care hospitals to their facilities: these patients must be documented “cleared” of MRSA. The concern – rightly – was that preventing the transmission of MRSA in the nursing home and community hospital setting would be difficult if not impossible, given the greater patient mobility and the reduced staff-to-patient ratio.
The result of all these activities? MRSA rates stayed the same across all the hospitals, unlike the efforts of the Northern European countries, western Australia, or UK in recent times. Some professionals viewed this as a qualified success (after all, MRSA rates did not increase!). However, my own view is that MRSA rates had reached a peak by then – mathematically and biologically, the probability that everyone that comes to a hospital will be infected by MRSA is negligible.
There were major problems with implementation of the infection control practices at that time. Most critically, there were insufficient isolation beds/rooms in the public sector hospitals. It was very quickly evident that there were more cases of MRSA infection (not even including cases of MRSA colonisation) than isolation rooms, and these rooms were also used to house patients with other transmissible diseases such as tuberculosis, chickenpox, etc. Setting aside “cohort” wards or areas for MRSA was also difficult to implement at that time. Tagging of MRSA cases also hit snags due to the computer systems of those times – inpatient and outpatient systems were not linked and MRSA-positive cases were often not identified in time. The nursing home/community hospital requirement for clearance of MRSA prior to patient transfer was the major “deal breaker” in MRSA control efforts. Many patients could not be transferred out of the acute care hospitals because of their MRSA status. I remember the frustration of those times – house officers and medical officers stymied by this clause in their efforts to discharge the patients from the acute care hospitals complained frequently and loudly, and I am sure a significant number took special efforts to ensure that the MRSA screening tests came back “negative”.
In the end, MOH had to step in to compel the nursing homes and community hospitals to accept MRSA-colonised/infected patients (or else the bottleneck in the acute care hospitals would never have cleared). Most acute care hospitals also took what were considered “practical” or “rational” decisions with regards to isolating MRSA-infected patients: only those with MRSA pneumonia or infected open wounds were isolated, in the (vain) belief that these were most likely the MRSA “super-spreaders”. You can probably still find local infection control staff who believe in this practice today. And the MRSA prevalence/numbers did not budge an inch.
However, even had there been fewer implementation issues, the chances of success in the initial MRSA control effort would have been miniscule. Below is a table of MRSA infection control guidelines that I had created as part of a master’s thesis.
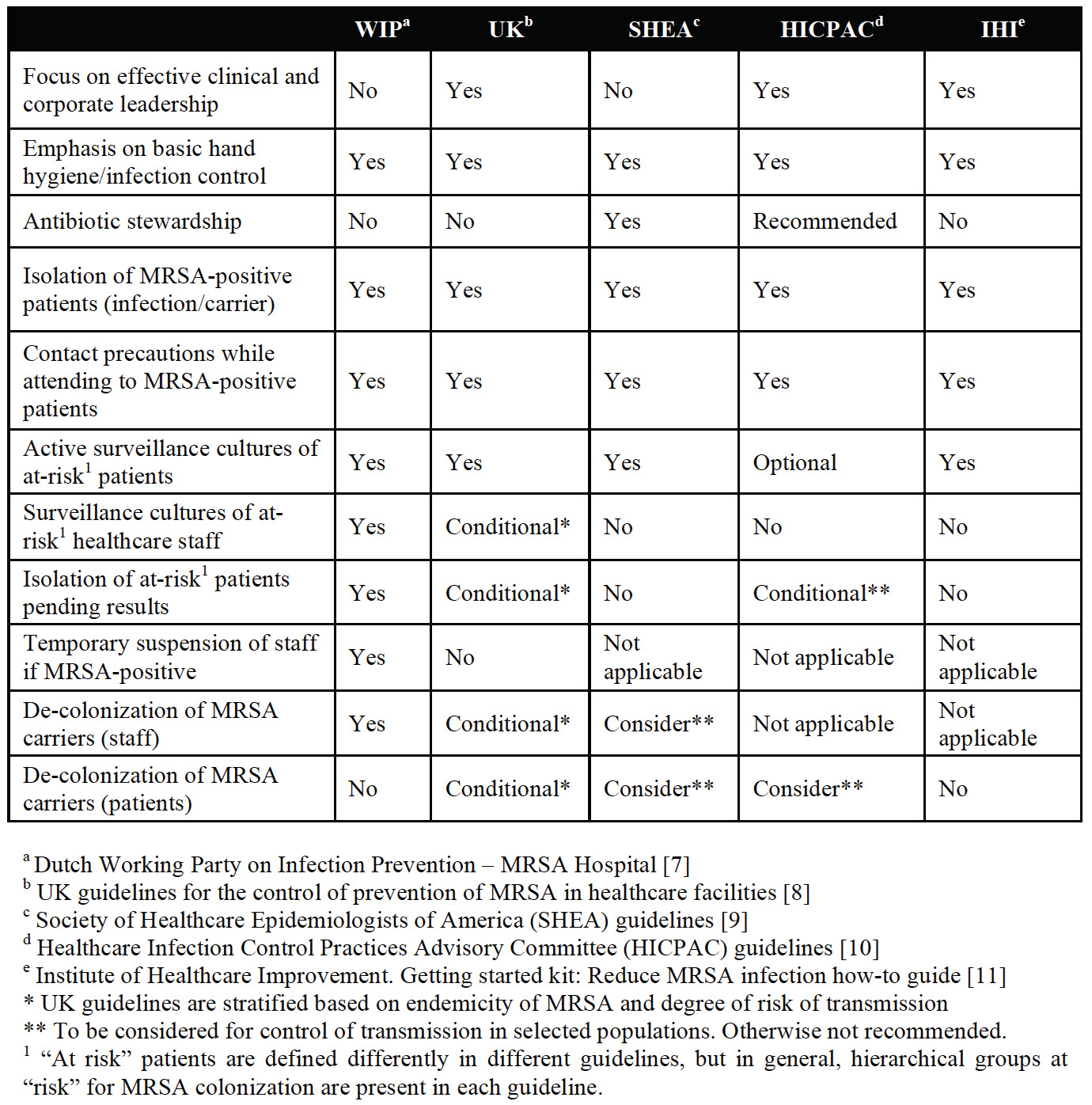
Table – MRSA infection control guidelines from various countries
All regions/countries with low MRSA rates in their hospitals have guidelines similar to WIP (Dutch Working Party on Infection Prevention – column 1 of the Table). The “extra mile” in terms of infection control practices involve:
- Isolating and screening patients at risk for MRSA colonisation upfront, with de-isolation only when proven negative for MRSA.
- Surveillance cultures performed on healthcare staff that are at risk for MRSA carriage (i.e. healthcare worker from overseas, or one that had tended to a patient with MRSA).
- Healthcare staff that are MRSA-positive are suspended from clinical duties until they have been de-colonised and proven negative for MRSA.
Of these, probably the first (screening for MRSA colonisation and isolating/cohorting colonised patients) is the most important and crucial first step, with the others being necessary in the subsequent efforts to drive MRSA rates down to zero. There is considerable controversy among infection control experts as to whether some/all of these last 3 measures are important. In theory, it is possible that with excellent hand hygiene among healthcare staff, and good contact precautions for MRSA-infected patients, MRSA can be controlled in the hospital setting. In practice, few institutions have matched the Scandinavian/Dutch/western Australia results without going the “extra mile”. Of these, the majority are private hospitals with mostly single rooms (i.e. only one patient per room) and where inpatient stay is short.
In any case, MRSA control efforts in Singapore languished after 1999 and had to be revived again 6-7 years later. Thousands of patients continued to be infected/colonised by MRSA in our hospitals in the interim.
