Clinical Vignette 19
This elderly gentleman had pulmonary tuberculosis 40 years ago. He was also a chronic smoker of 60-odd years, smoking at least 10 cigarettes a day. He presented with paroxysmal coughing for 2 days (more than his usual “smoker’s cough”), accompanied initially by rusty, blood-streaked sputum, but developed frank hemoptysis (coughing out bright red blood) in the two hours prior to his visit to the hospital emergency department. He did not have fever, and his chest X-ray is shown below.

Chest X-ray of the elderly gentleman with prior tuberculosis and current hemoptysis.
Question: What is the diagnosis and how would you prove it?
[Updated 7th February 2015]
The diagnosis is pulmonary aspergilloma. One can just about imagine a “ball” at the medial aspect of the old TB cavity.
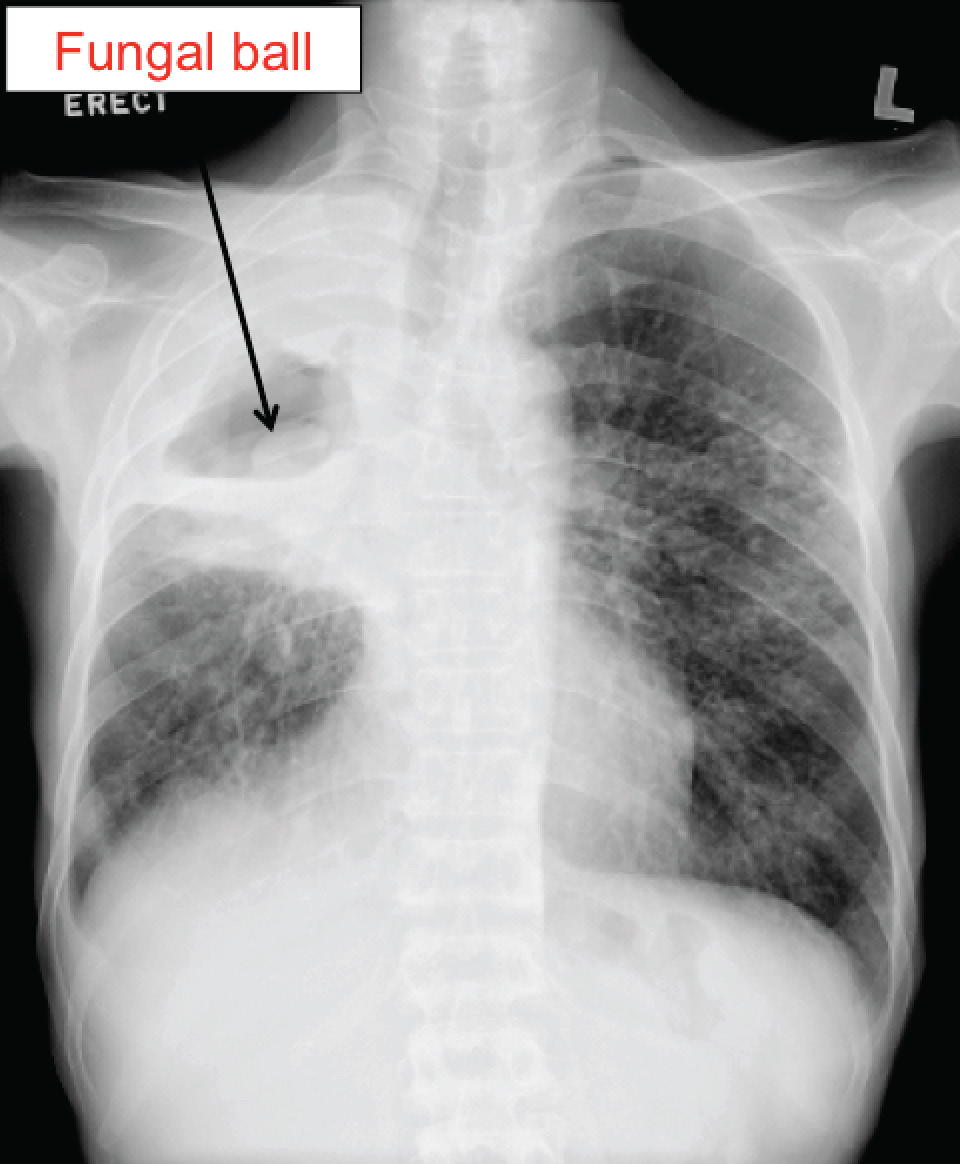
Arrow shows the suspected fungal ball.
The classical way to make the diagnosis is to have the chest X-ray taken with the patient in a different position, as fungal balls are generally mobile and will shift its position according to gravity. Here (below) is an image of the same patient lying in the right lateral recumbent position.

Chest X-ray with patient in the right lateral recumbent position. The fungal ball has “fallen” by gravity.
Most pulmonary aspergillomas are asymptomatic. However, hemoptysis can occur due to the surrounding reactive vascular granulation tissue, or when there is invasion into a bronchial artery. The latter can be life-threatening. Antifungal therapy does not have much effect, probably because drug penetration into the cavity is extremely poor. Surgical resection is the mainstay of therapy for a fungal ball causing severe hemoptysis, with bronchial artery embolisation occasionally performed mainly to “buy time” for organising the surgery.
