Clinical Vignette 24
A middle-aged woman underwent chemotherapy after being diagnosed with acute lymphoblastic leukaemia (ALL). She was re-admitted 4 days post-completion of #1A and #1B hyperCVAD with septic shock requiring dopamine support. Her absolute neutrophil count (ANC) was 0.02 and her initial chest X-ray was normal. She was treated with intravenous (IV) imipenem as per protocol, and blood cultures grew Pseudomonas aeruginosa that was susceptible to all anti-pseudomonal antibiotics. Her fever resolved on the second day of hospitalisation and she was weaned off inotropic support at the same time.
The antibiotic therapy was de-escalated to IV piperacillin/tazobactam on the third day of hospitalisation. However, she had a recurrence of fever on Day 4 of hospitalisation, associated with left-sided chest pain and breathlessness, requiring intra-nasal oxygen support (4 L/min). Her chest X-ray showed new left lower zone infiltrates (Figure 1 below) and she remained profoundly neutropenic at this point.
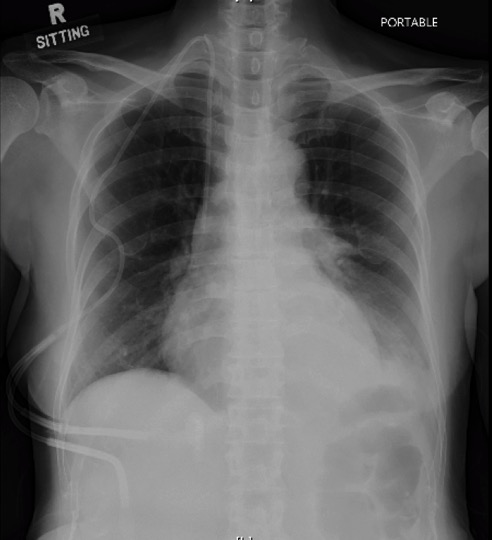
Figure 1. Chest X-ray of neutropenic patient with ALL, showing left lower zone infiltrates.
Her antibiotic therapy was escalated to IV imipenem with IV gentamicin, and a CT thorax was arranged (Figure 2 below), which showed dense consolidation of the left lower lobe.
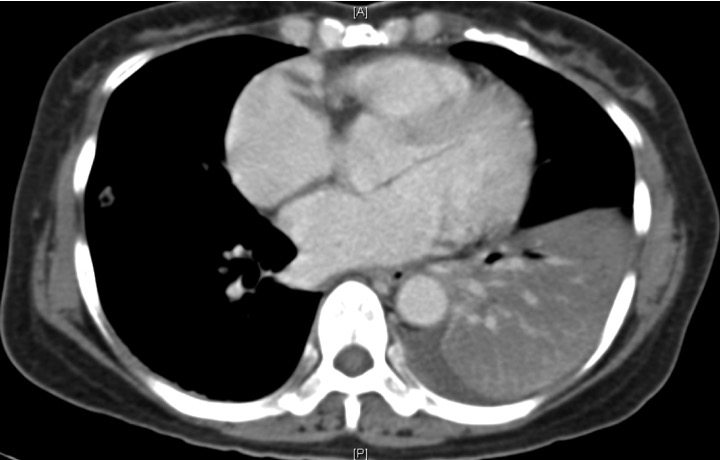
CT image of neutropenic woman with ALL, showing dense consolidation of the left lower lobe.
Repeat blood cultures were negative at this point.
Question: What is the likely causative organism for this patient’s chest infection?
[Updated 21st March 2015]
This is currently a rare clinical presentation, but nonetheless “classical”. Most clinicians would assume that invasive fungal infections (IFIs) would be high on the cards, given the profound neutropenia and antibiotic coverage. However, it is extremely unusual for IFIs to present so acutely, with actual clinical deterioration and de-saturation on just the 4th day of febrile neutropenia. The large consolidation seen on the CT thorax is also very atypical of an IFI, which usually appears as nodules – occasionally with “crescent” and “halo” signs – on CT.
Such a presentation is invariably Pseudomonas aeruginosa pneumonia. I am not certain how to explain the process pathologically, but the clinical deterioration and appearance of lung consolidation(s) after a short period of clinical improvement is typical. Such patients need careful management and support. It is unclear at present whether the addition (or change) of anti-pseudomonal antibiotics will improve outcomes.
