Clinical Vignette 27
A middle-aged man who had renal transplantation 5 years ago (but otherwise well) presented with fever and shortness of breath for 2 weeks. He was found to have a right pleural effusion on chest X-ray, and underwent a diagnostic pleural tap. The TB PCR was positive from the pleural fluid, and he was started on standard anti-tuberculosis therapy (but with levofloxacin substituted for rifampicin owing to the interactions of the latter drug with other agents taken to maintain the renal transplant). The initial chest X-ray and the subsequent chest X-ray taken 10 days later are shown below.
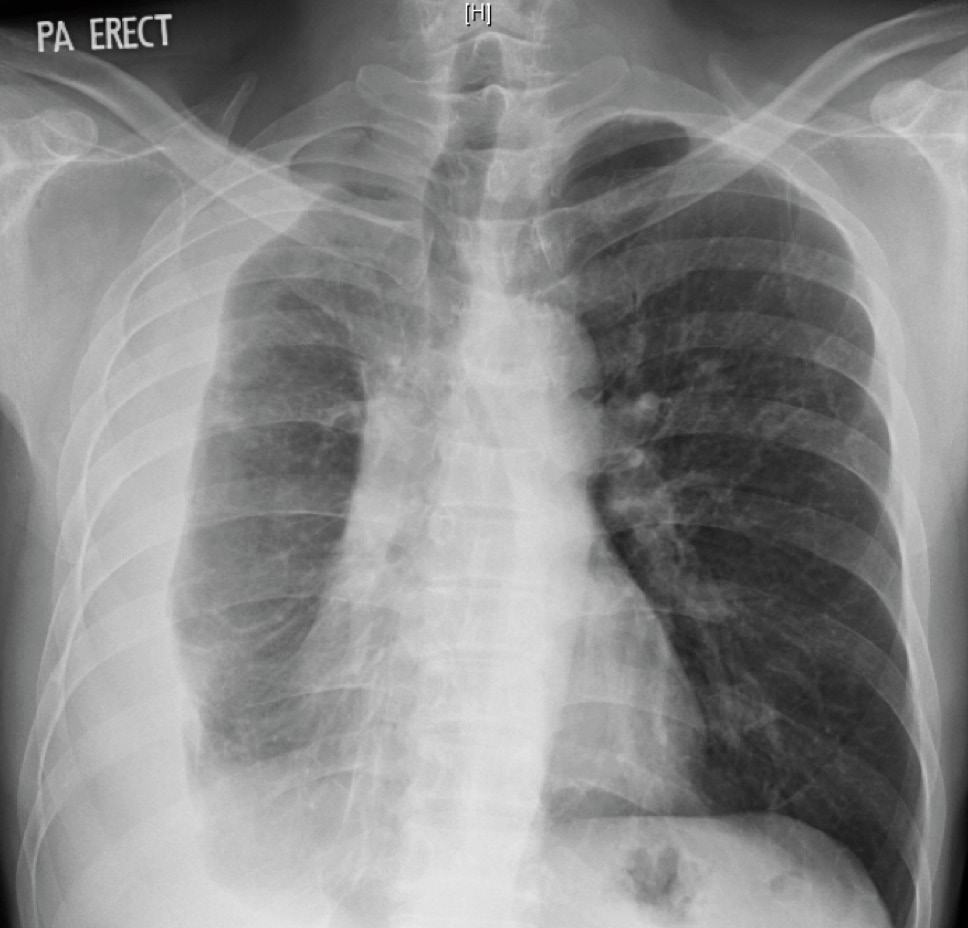
Initial chest X-ray of the man with renal transplant, showing a right-sided loculated pleural effusion.
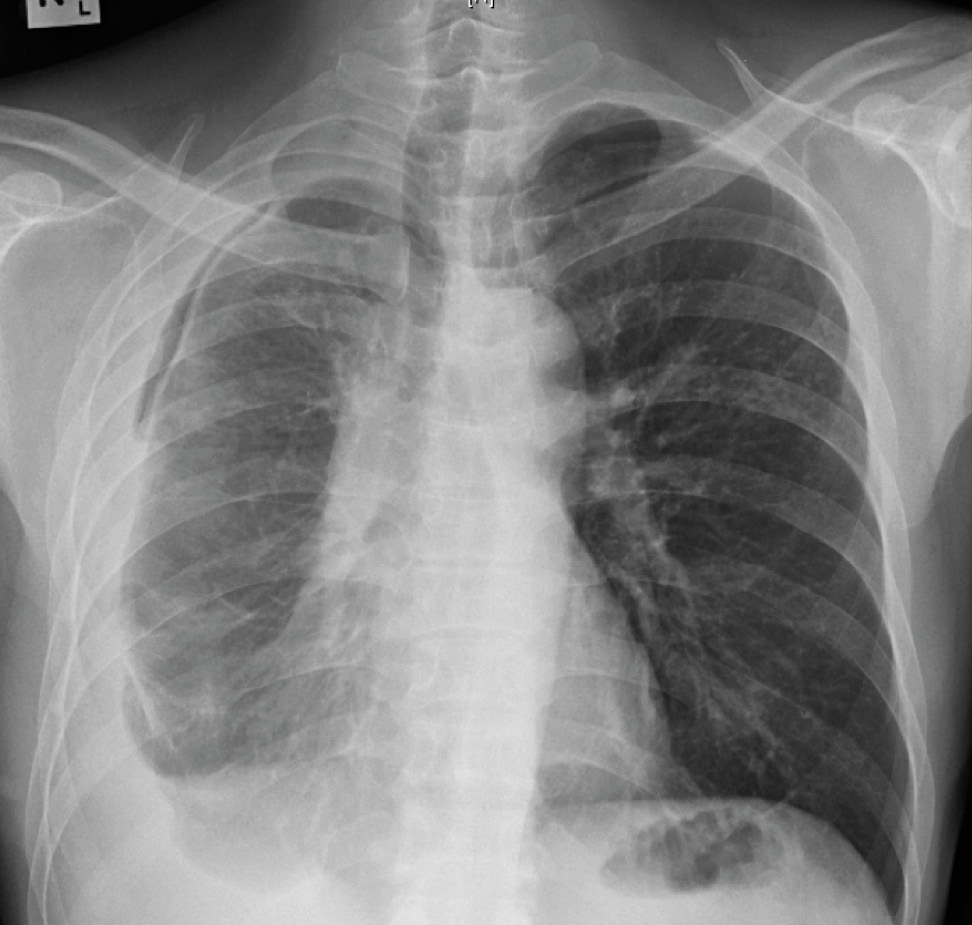
Chest X-ray taken 10 days later, after a diagnostic pleural tap and drainage had been performed.
He felt clinically better after starting the anti-tuberculosis therapy, with no further fever nor shortness of breath (except on exertion), and had also started to gain weight. The pleural fluid culture was positive for Mycobacterium tuberculosis complex which was sensitive to all drugs. During the routine follow-up visit after completing 2 months of therapy, however, the chest X-ray was grossly abnormal.
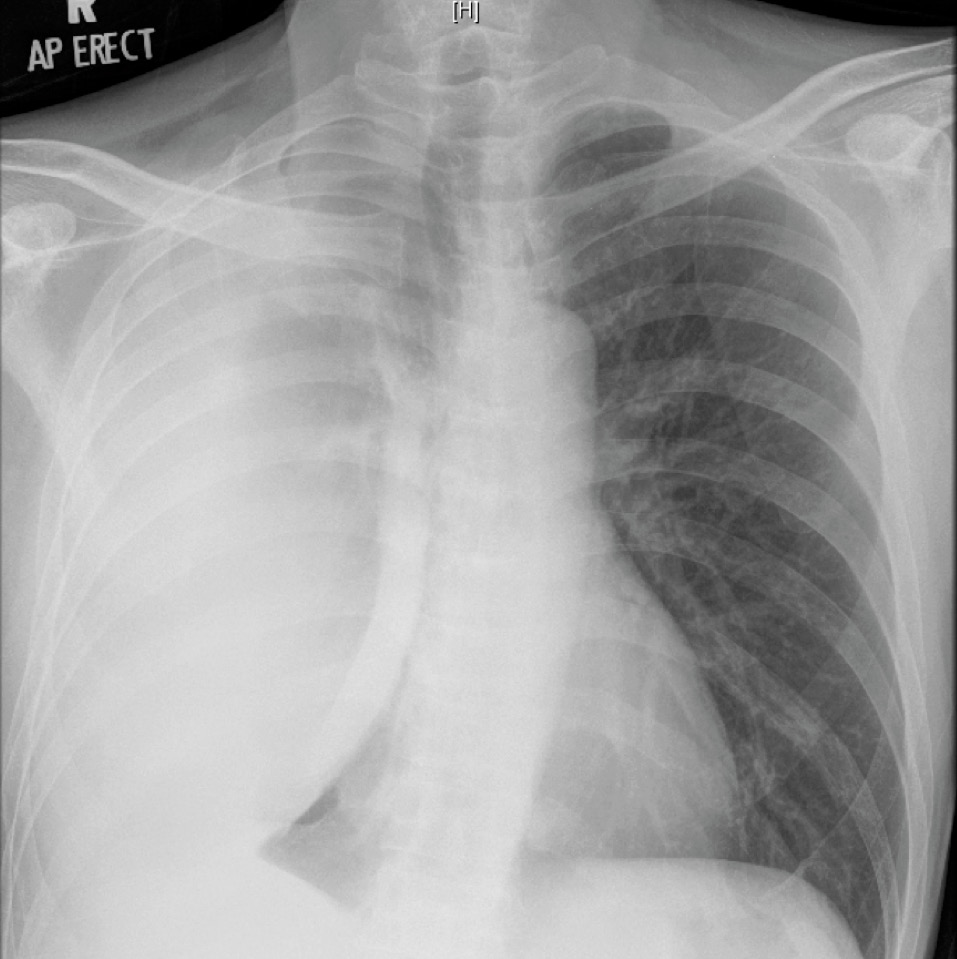
Chest X-ray 2 months after starting anti-tuberculosis therapy, showing a massive right pleural effusion.
Question: What is the diagnosis and how should the patient be managed?
[Updated 11th April 2014]
This patient had a loculated pleural effusion with radiological suggestion of a trapped lung. However, the massive increase in size of the pleural effusion 2 months after starting appropriate treatment is consistent with a paradoxical response to anti-tuberculosis therapy. This is now believed to be a immune reconstitution syndrome, and occurs in up to 15% of non-HIV patients but up to 25% of HIV-infected patients with concurrent tuberculosis who are started on highly-active anti-retroviral therapy (HAART). It occurs more commonly with extra-pulmonary tuberculosis, particularly cervical lymphadenitis and TB pleurisy.
Treatment of paradoxical response to anti-tuberculosis therapy is largely conservative, although steroids and/or surgical therapy are options if symptoms are severe. We offered the patient surgical drainage of the effusion in view of its massive size (potentially complicating respiratory function should any new lung infection develop), but he wisely refused. Subsequent chest X-rays showed gradual reduction in the size of the effusion over time, although it did not really disappear even at the time of stopping anti-tuberculosis therapy.
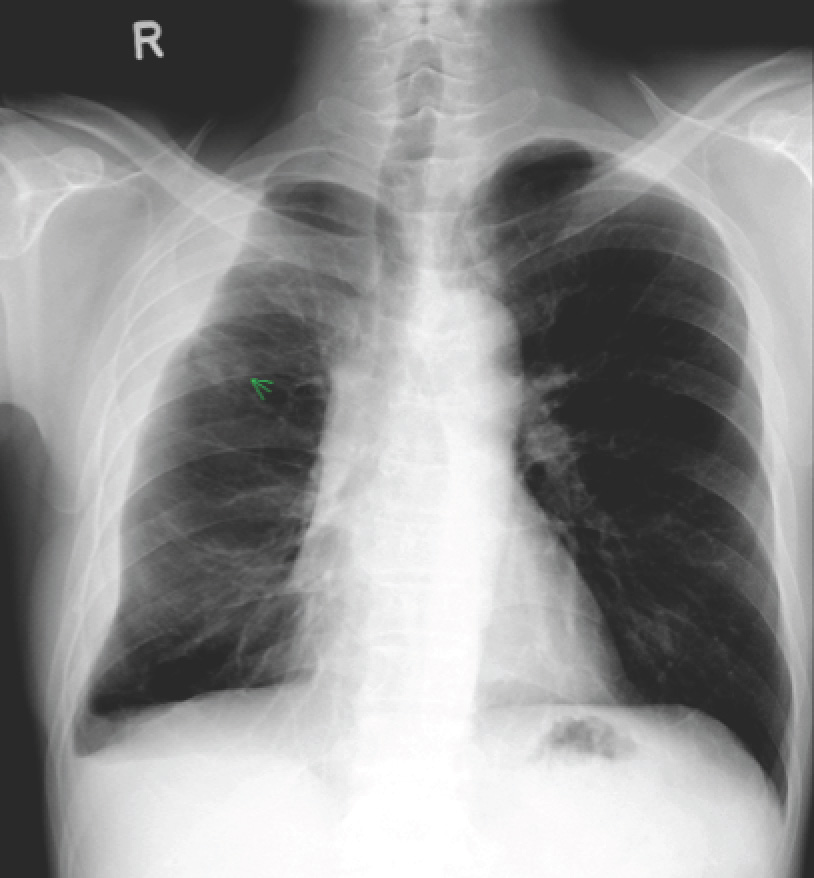
Chest X-ray of the patient with TB pleural effusion and paradoxical response to therapy one year after starting TB treatment.
