Clostridium difficile
Clostridium difficile is an anaerobic Gram-positive rod that can colonise the intestines of humans and other animals. It is related to the bacterium that causes tetanus (Clostridium tetani) as well as the bacterium that causes food poisoning and occasionally gas gangrene (Clostridium perfringens). Like all Clostridia, it can form spores, which it does as a survival response to adverse changes in its environment. It is best known for its ability to cause diarrhoea via the production of its two exotoxins – toxin A (TcdA) and B (TcdB), particularly in patients who have received extended courses of broad-spectrum antibiotics within the hospital environment.
An excellent review on Clostridium difficile infections was published today in the New England Journal of Medicine (NEJM). It is unfortunately behind the NEJM paywall, but the salient points are as follows:
- Risk factors for colonisation (and disease) include advanced age, cancer chemotherapy, severe underlying disease, and other factors that affect the faecal microbiome (i.e. antibiotics).
- Infants may be colonised by C. difficile, but are mostly asymptomatic, likely because of the lack of the toxin-binding receptors in the infant gut.
- The organism is otherwise non-invasive, with rare reports of infection outside the gut.
- One particular strain of C. difficile – the BI/NAP1/027 strain (a complicated nomenclature that includes the results of 3 different typing methods) – is associated with higher mortality rate (3 times relative to other C. difficile strains).
- The immune response appears to be due to antibody production directed against TcdA and TcdB – and passive immunisation with monoclonal antibodies against these two toxins has resulted in reduced recurrence rates.
- C. difficile rates may fluctuate greatly each year, but appear to be generally increasing in the U.S. Community-acquired infections are also on the rise.
- Diagnosis appears problematic – DNA assays are highly sensitive but may detect clinically insignificant infection. However, toxin assays are less sensitive and culture-based methods are difficult to perform and not widely available.
- Stool testing should only be limited to patients with diarrhoea, and does not appear to be important for infection control (i.e. surveillance testing in patients without diarrhoea has not been shown to be useful).
- Prevention has mainly been in the form of antimicrobial stewardship and isolation of patients with C. difficile colitis.
- Treatment is classically with metronidazole or vancomycin, although oral vancomycin has been shown to be more effective compared to metronidazole.
- Fidaxomicin (not available in Singapore) appears to be particularly useful at reducing the risk of recurrence with infections caused by the BI/NAP1/027 strain.
- Fecal microbial transplantation has been shown to be very effective in cases of recurrent colitis.
What is the situation in Singapore? Unfortunately, we only have a rather patchy picture – the latest data are behind the “MOH firewall”, and is much harder to access than articles behind journal “paywalls”!
In 2002-2003, the incidence of C. difficile infections at the Singapore General Hospital was approximately 53.8 cases per 100,000 inpatient-days. This was published in the journal Pathology in 2007 (behind yet another paywall). Then investigators from Tan Tock Seng Hospital showed that the incidence of C. difficile infections had increased dramatically from 2001 to 2006, rising to just below 70 cases per 100,000 inpatient-days.
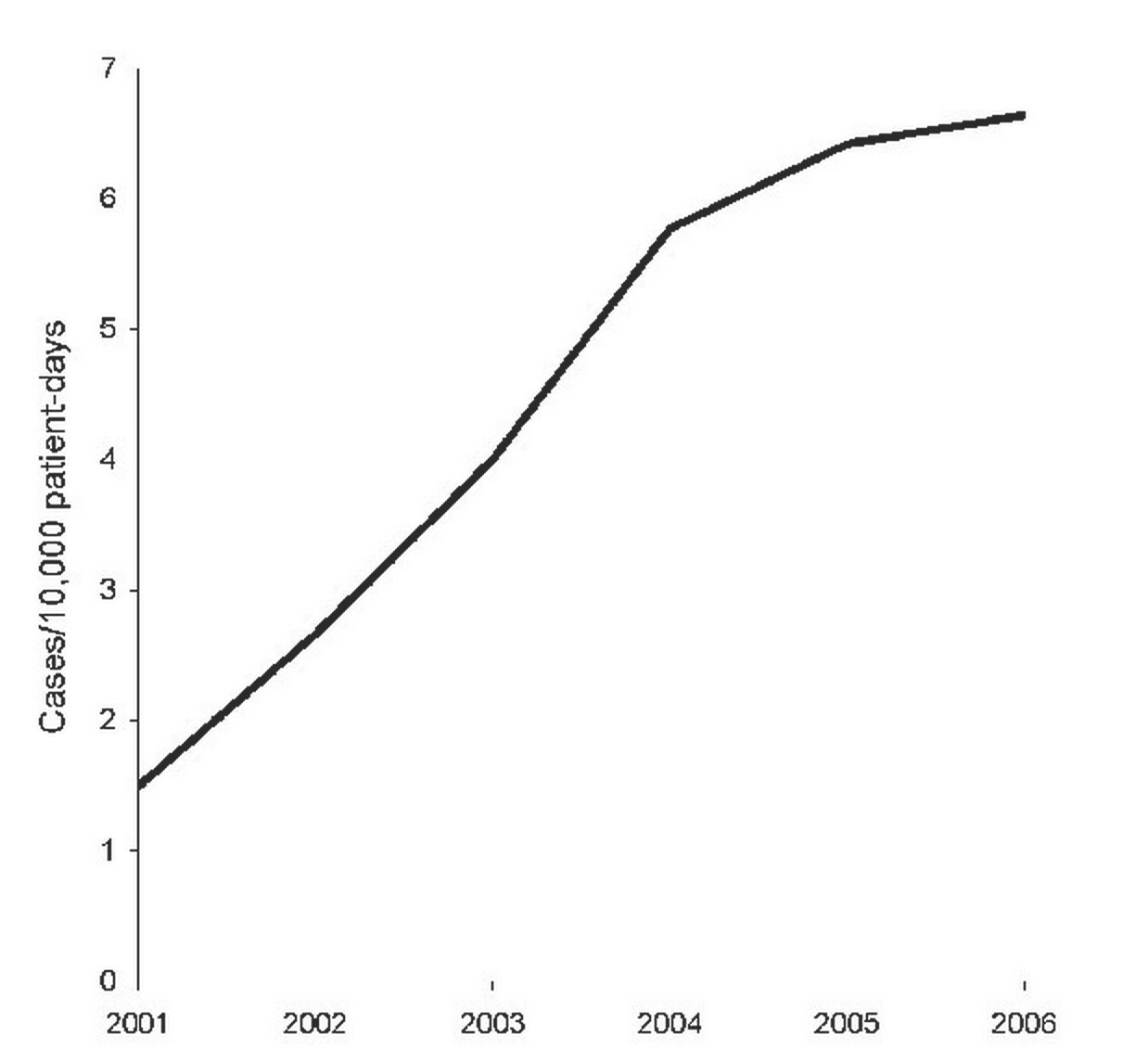
Rise in Clostridium difficile infections at TTSH between 2001-2006 (figure from Emerging Infectious Diseases).
As one of the functions of the National Antimicrobial Resistance Surveillance (Singapore) programme, or NARSS for short, we surveyed C. difficile rates in 3 Singaporean hospitals (SGH, TTSH and CGH) and found somewhat to our amazement that infection rates had fallen between 2006 to 2008 to a low of approximately 30 cases per 100,000 inpatient-days. This result occurred despite a dramatic rise in the number of C. difficile tests ordered – the latter being likely a function of increased awareness among the clinicians.
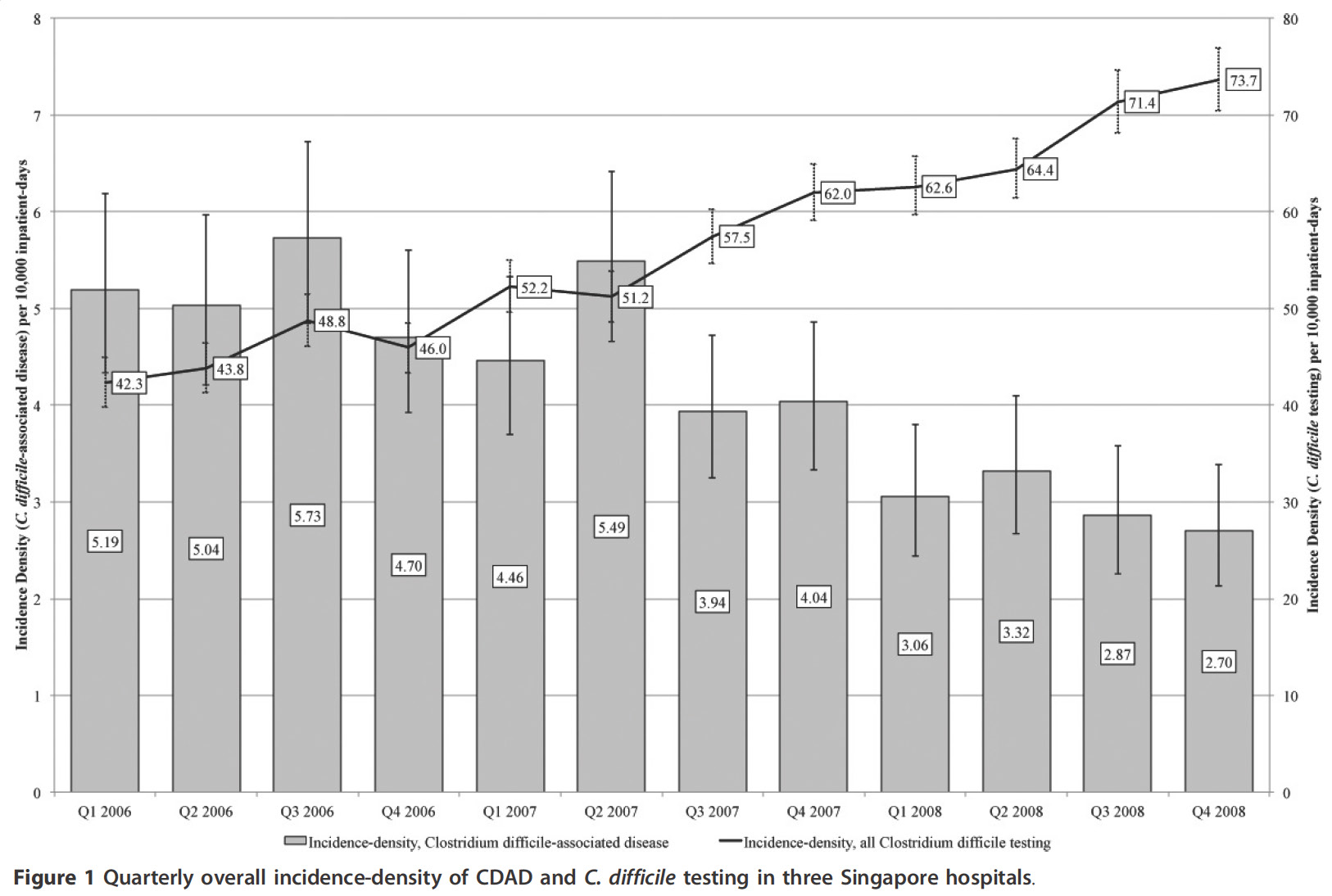
Falling Clostridium difficile incidence in 3 Singaporean hospitals, 2006-2008 (figure from BMC Research Notes).
It is likely that the incidence of C. difficile infections in Singapore has risen again since 2008, although it is not publicly known by how much. A large study looking for the BI/NAP1/027 strain was performed between September 2008 and December 2009, sponsored by the Ministry of Health, and this found that only 3 of 272 viable C. difficile isolates obtained from local hospitals had to PCR027 ribotype (and all 3 patients were relatively well, unlike international reports). However these isolates were susceptible to moxifloxacin, which would be atypical of the epidemic BI/NAP1/027 strain. The hypothesis that these 3 isolates are not really part of the global epidemic strains was confirmed in a global C. difficile BI/NAP1/027 whole genome sequencing study, which showed that these isolates were outside of the two major epidemic lineages (the SGH microbiology blog‘s chief blogger contributed the strains to this global study). Community-onset infections were noticed at the National University Hospital, and a small study was performed between December 2011 and May 2012 which showed that virtually all but one (of 33) community-onset cases had some degree of healthcare exposure. Unfortunately, these last study results are behind a paywall.
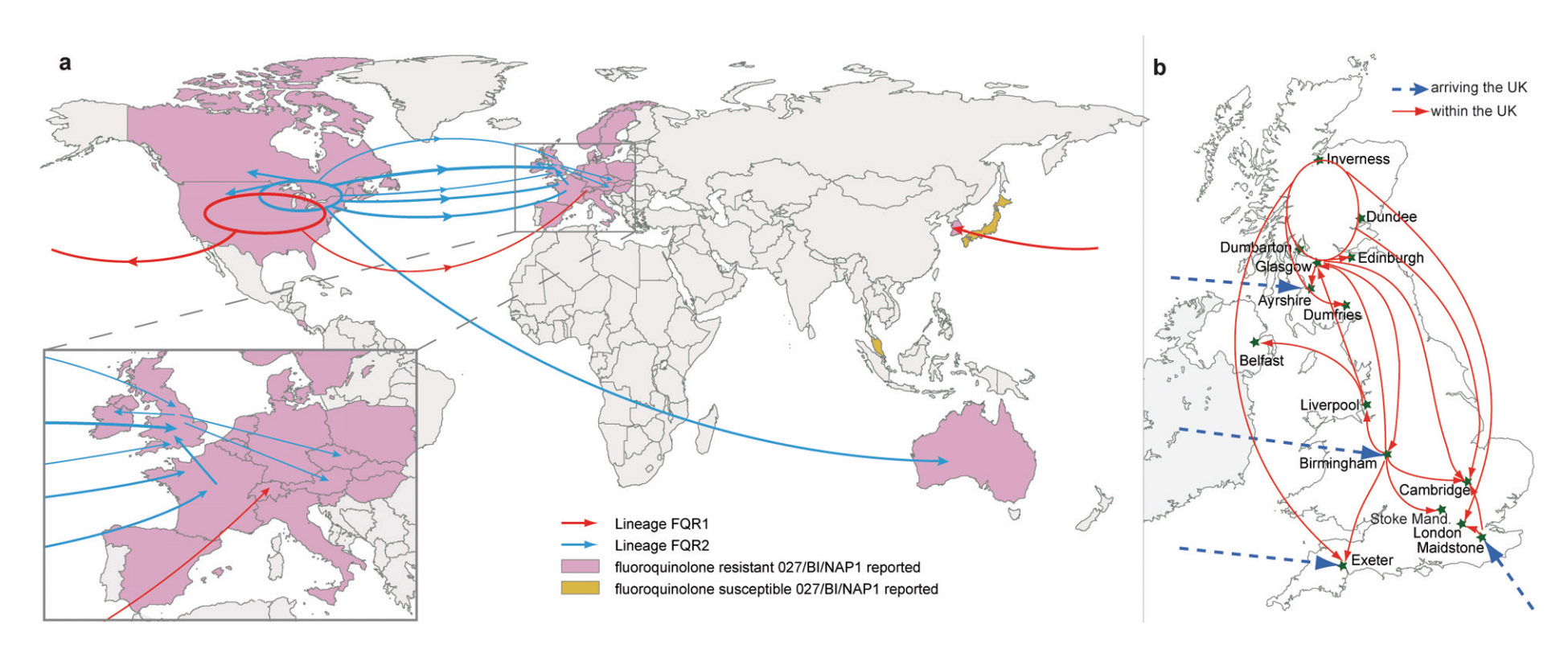
Map showing the inferred transmission events for the BI/NAP1/027 epidemic strains of Clostridium difficile (Singapore contributed strains to the study). This map was obtained from the Nature Genetics publication.
There are no local consensus guidelines for treatment, although nearly all clinicians would use either metronidazole or oral vancomycin for significant C. difficile colitis. NUH has set up a fecal transplant service since 2014, but the number of patients treated thus far has been small.
