Clinical Vignette 29
An elderly man who was 4 years post-coronary artery bypass grafting developed fever for a week, which he initially ignored as being “just a flu”. However, he developed central chest pain on the 7th day of fever, and was admitted to a local hospital.
His WBC was 6,700 cells per mcL (65% neutrophils). The blood cultures flagged positive for a Gram-negative rod and the admission chest X-ray is shown below.

Chest X-ray of the elderly gentleman with chest pain.
Question: What is the likely identity of the Gram-negative rod and what is the diagnosis here?
[Updated 25th April 2015]
A rather difficult case to guess, perhaps. But this patient had a normal WBC with normal differential counts despite having Gram-negative bacteraemia, and one of the few types of Gram-negative rods where such a phenomenon is observed is Salmonella spp. Given the elderly patient and the aortic dissection seen on the chest X-ray, this is likely non-typhoidal Salmonella bacteraemia with infected aortic aneurysm/dissection. A CT image is shown below.
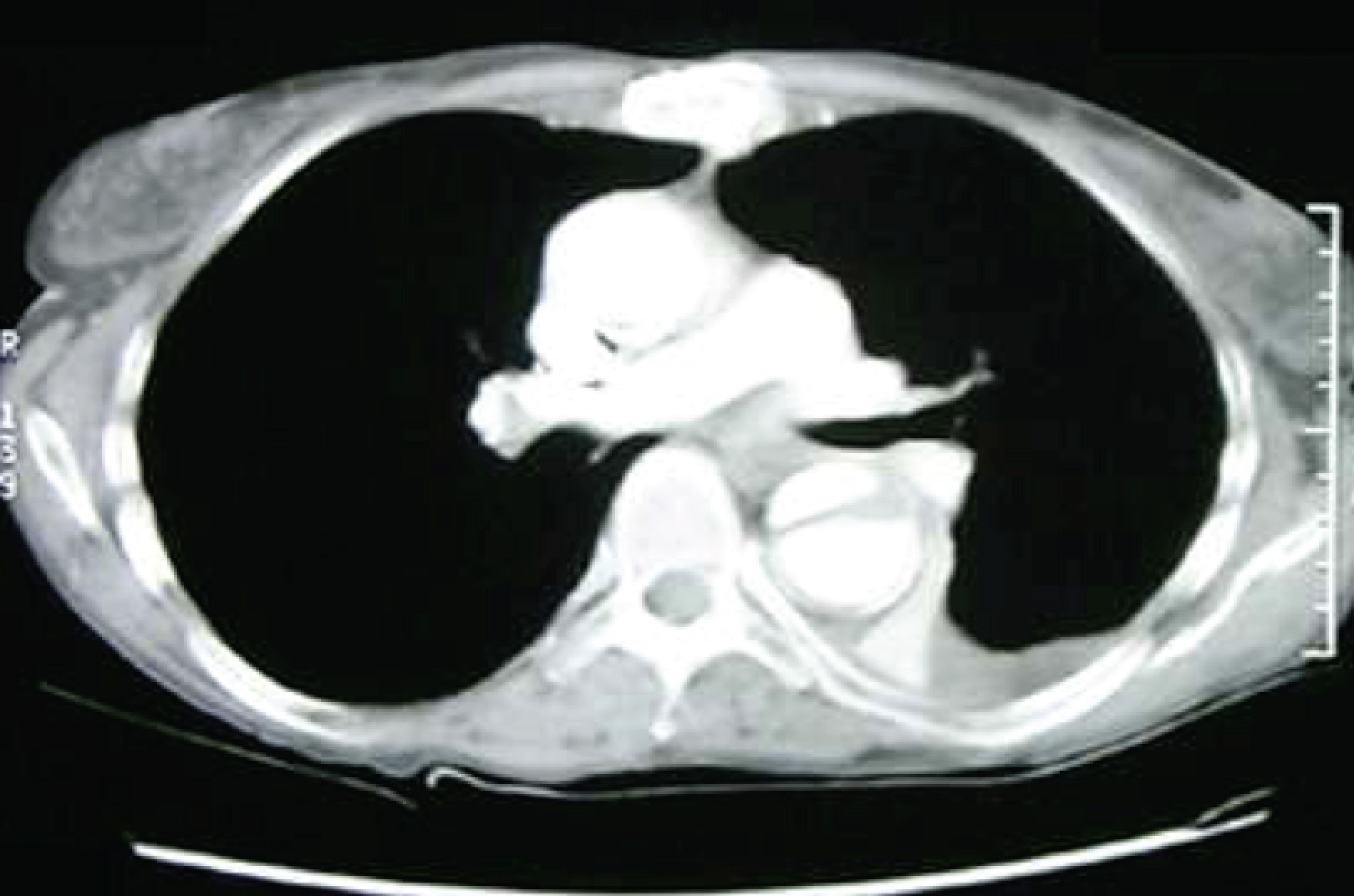
CT thorax image showing the aortic dissection, with a larger false lumen.
Management is surgical (as for any aortic dissection) and a prolonged course of antibiotics. There is likely no difference in outcomes between oral and IV antibiotics for the treatment of this condition.

Serogroup or serotype?
LikeLiked by 1 person
Hello, Prof Chiu!
In Singapore, it is almost always Salmonella enteritides (Group D).
LikeLike