Clinical Vignette 32
A middle-aged housewife who was previously well presented with high fever for 2 days, waking up drowsy and disoriented on the second day. On clinical examination, she was febrile and her conscious state was impaired (GCS: E3 V4 M5) – she was unable to answer questions appropriately, opened eyes only on calling, and was unable to follow commands consistently. Her neck was supple and she had no rash; there were no other abnormal clinical findings.
Her daughter (in Primary school) had an upper respiratory tract infection a week ago, but there was no other significant contact or travel history. A CT head was normal. She was transferred to the Neurological High-Dependency Unit for monitoring, and a lumbar puncture and MRI of the brain was arranged.
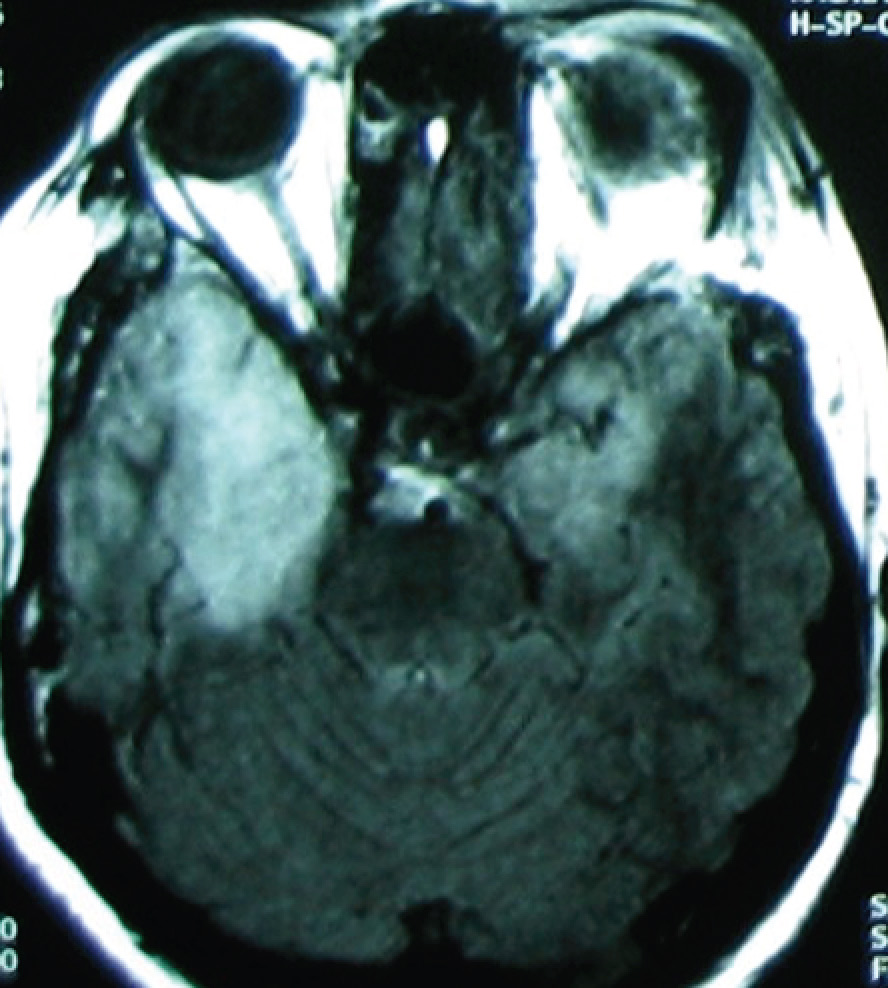
MRI (T2 image) of the woman with fever and impaired consciousness.
Question: What is the diagnosis and how should she be managed?
[Updated 16th May 2015]
Her symptoms are typical of encephalitis, and the MRI shows enhancement of both (right more than left) temporal lobes of the brain. This is virtually pathognomonic of herpes simplex type I (HSV-1) encephalitis. It is unclear at this point in time why the virus acutely infects the brain in a small proportion of patients (but not others). The majority of patients will not have the typical oral-mucosal herpetic vesicles or ulcers that are seen with HSV-1 infection. The diagnosis can be confirmed via lumbar puncture, with cerebrospinal fluid (CSF) sent for HSV PCR. This is in addition to other CSF tests such as CSF analysis, etc (in order to be complete – CSF is much harder to obtain than blood).
Treatment is with intravenous (IV) acyclovir. Medscape has a nice overview of the condition.
