Tuberculosis: Legal Aspects in Singapore
The standard short-course therapy for pulmonary tuberculosis involves taking 4 to 5 different medications for 6 months, and both duration of therapy and medication count (normally about 10 or so pills each day) can be significantly increased as a consequence of drug resistance and/or drug intolerance requiring a change of regimen. Compliance to anti-tuberculosis therapy can therefore be difficult even without factoring in other possible social, personal and medical issues. However, non-compliance to anti-tuberculosis therapy is not the same as non-compliance to hypertension, diabetes mellitus or cardiovascular disease therapy – only the person who is non-compliant for the latter conditions is potentially harmed (perhaps his/her family and friends as well, in a smaller degree). Persons who are non-compliant to anti-tuberculosis therapy may affect both themselves and the community in the form of higher rates of treatment failure, relapse and emergence of drug resistance, and increased transmission of tuberculosis.
In view of the potential public health threat of tuberculosis transmission, legal interventions culminating in detention or incarceration for completion of anti-tuberculosis therapy remain important in the overall public health framework for the control of tuberculosis. They have been criticised as being based on limited evidence, although more recent publications suggest that such measures improve treatment completion rates, albeit the question of cost-effectiveness remains difficult to address. Legal interventions – particularly incarceration – rightly remain an option of last resort in most developed countries.
In Singapore, the Tuberculosis Control Unit (TBCU) actively engages patients who are non-compliant to anti-tuberculosis therapy, employing a variety of measures to determine and address the reasons for non-compliance. Such measures include but are not limited to counselling, medical social worker review for assistance with financial and social problems, and the provision of supermarket vouchers sponsored by SATAComm Health – a local non-governmental organization – for those who subsequently adhere to directly observed therapy (DOT). Nonetheless, there remain patients that continue to be non-compliant despite these efforts. These recalcitrant patients are evaluated by the Committee for TB Treatment Defaulters, established since 2004 with members appointed by the Ministry of Health (MOH), that makes recommendations to the Director of Medical Services (DMS – the top “ranking” doctor in MOH Singapore) whether the aforementioned patients should undergo compulsory DOT until completion of therapy. The MOH will then serve legal orders to the patients under the Infectious Disease (ID) Act, where patients are ordered to comply or else face fines (up to SGD10,000) and/or imprisonment (up to one year). There are two relevant levels of the ID Act : Section 8(1) and Section 15(1). Section 8(1) states that the DMS may require any person with an infectious disease to submit to medical examination or treatment, whereas Section 15(1) states that the DMS may order any person with an infectious disease to be detained and isolated in a hospital or other place for a period of time and under conditions to be determined by the DMS.
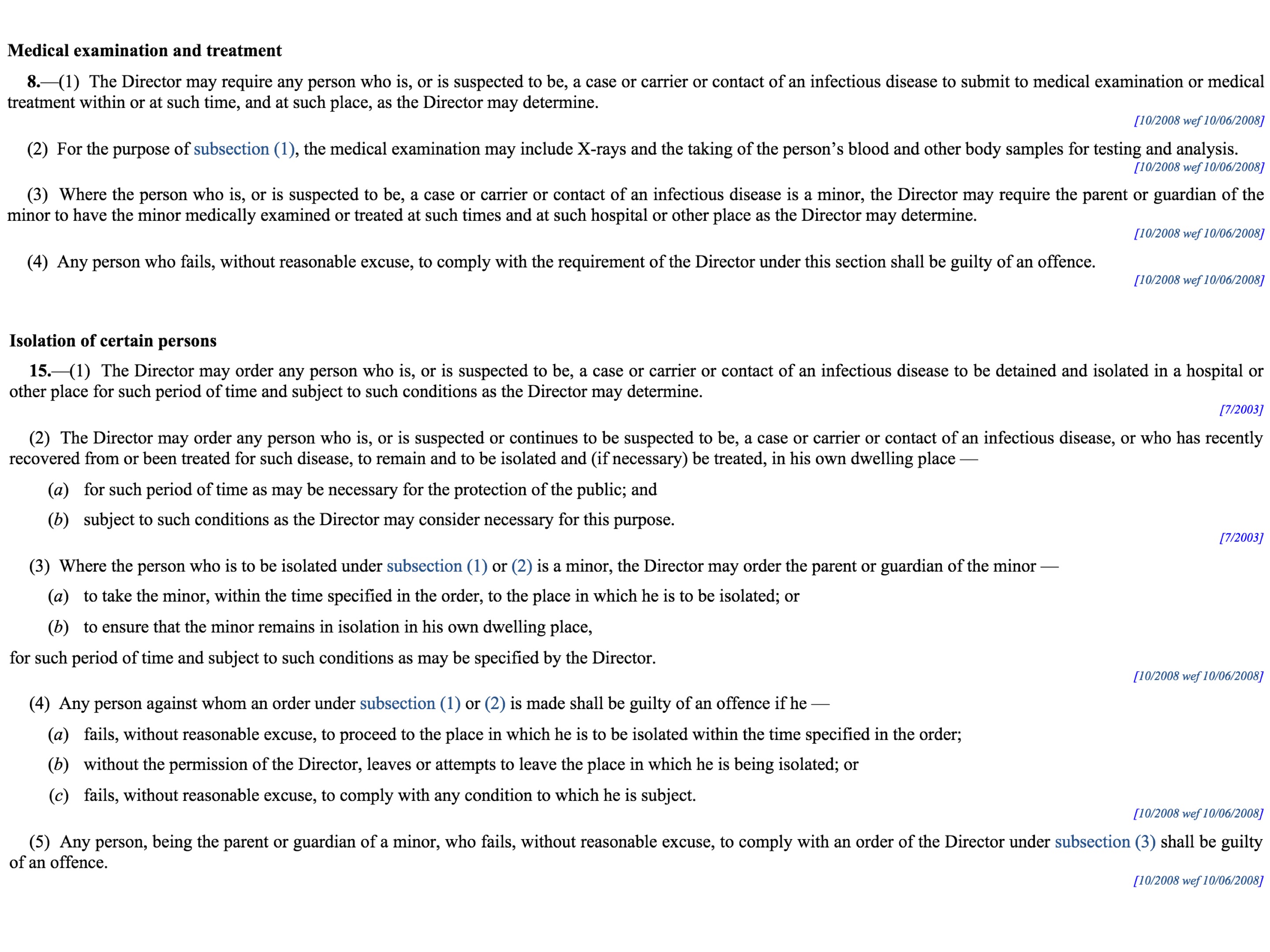
Sections 8 and 15 of the ID Act, Singapore
However, I am unaware that anyone has ever been charged under the ID Act for being non-compliant to anti-tuberculosis therapy, and there has also been no publications to date on the success of the legal orders in improving compliance to therapy locally. It would be good to know the results, not least because the dynamic between public health and individual liberties are increasingly under scrutiny and challenge, even in Singapore. Also, tuberculosis, unlike Ebola or SARS, does not seem likely to elicit the kind of visceral response that would result in overwhelming public support for the involuntary incarceration of treatment-recalcitrant persons (except perhaps for persons with extensively drug-resistant tuberculosis, or XDR-TB for short).

[…] infectious diseases at Changi General Hospital – had commented in response to my earlier post on legal aspects of tuberculosis management that one other challenging issue sometimes faced by doctors was with regards to air travel and […]
LikeLike