MERS-CoV, South Korea, 2015
The evolving outbreak of the Middle-East respiratory syndrome coronavirus (MERS-CoV) in South Korea is the largest to date outside the Middle Eastern countries, involving 12 persons to date (including one that had – ignoring the advice of South Korean health officials – flown to Hong Kong on 26th May and then to Huizhou via Shenzhen on 27th May). The index case was a 68-year-old man who had traveled extensively through various parts of the Middle East (Bahrain, United Arab Emirates, Saudi Arabia, and Qatar) between 18th April and 3rd May on farming-related business before returning to South Korea on 4th May, and developing symptoms on 11th May. He had sought outpatient treatment between 12th-15th May, was hospitalised between 15th-17th May at one hospital, discharged, and re-admitted on the same evening to a second hospital. He tested positive for MERS-CoV on 20th May and was transferred to the designated national isolation and treatment facility for further management. The eleven secondary cases acquired the virus largely as a consequence of nosocomial transmission – a more detailed report can be found on the ECDC website here.
There are 1,172 cases as of 30th May 2015 (1,134 in the Middle-Eastern countries) with 479 deaths (case fatality rate of 40.9%). The latest ECDC epidemiology report has a beautiful map geographic distribution of confirmed MERS-CoV cases and likely source of origin, which I have taken the liberty to reproduce below.
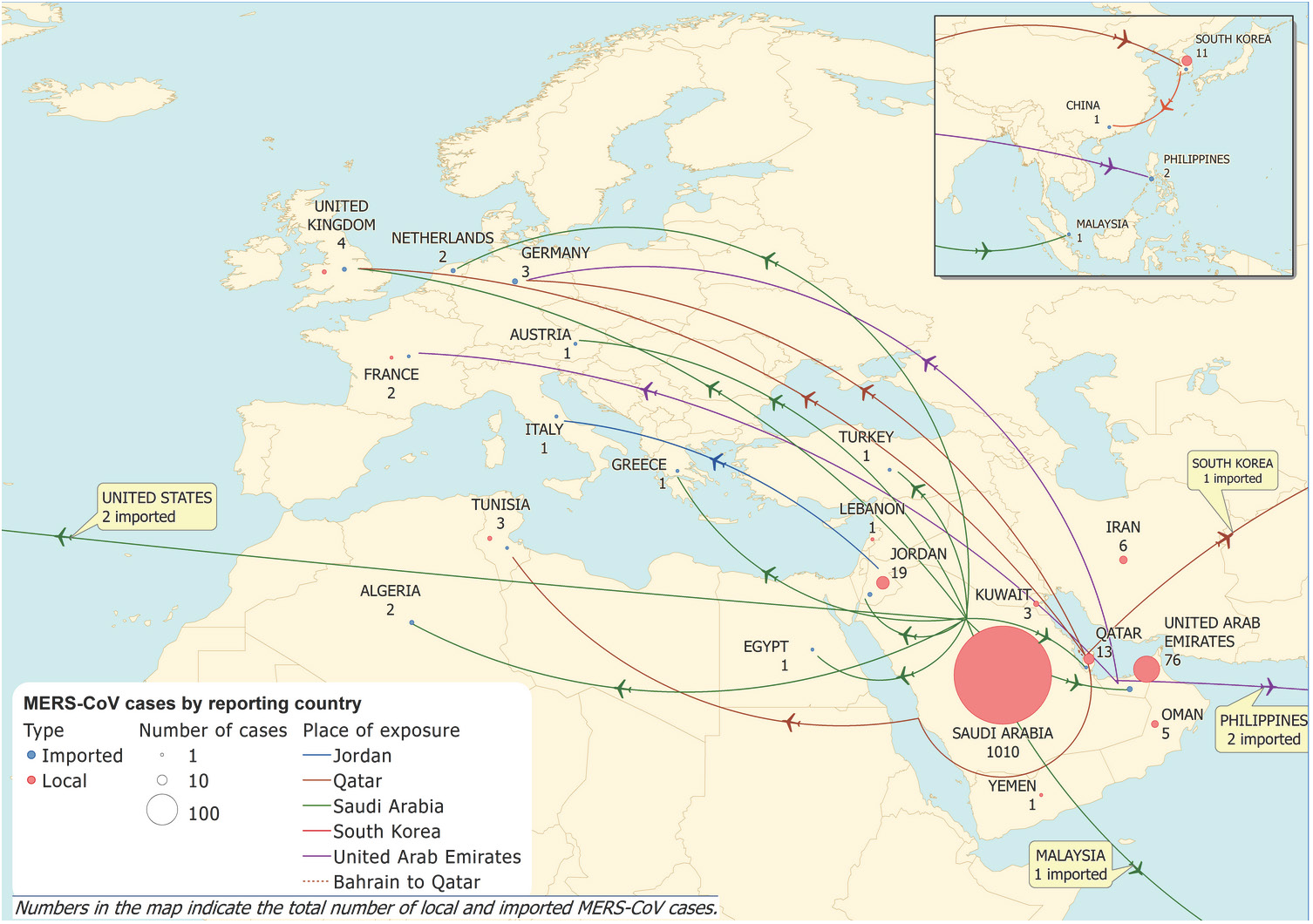
Map of confirmed MERS-CoV cases and probable origin of infection, as on 29th May 2015. This map was produced by the ECDC and published in their epidemiological update on 30th May 2015.
Although distinct from the severe acute respiratory syndrome coronavirus (SARS-CoV) genetically, the two viruses share several similarities, including:
- Origin in bats (Chinese horseshoe bat for SARS-CoV and the Egyptian tomb bat for MERS-CoV), although other animals were more commonly involved in the initial zoonotic transmissions (civet cat and possibly rats for SARS-CoV and camels for MERS-CoV).
- Respiratory system involvement.
- High case-fatality rate.
- Unsustained and rather inefficient human-to-human transmission, with most such events occurring in hospitals.
Singapore remains vulnerable to importation of the MERS-CoV because of the many visitors (including medical tourists) from the Middle East, and also because many Singaporeans regularly visit Saudi Arabia on Hajj and Umrah pilgrimages, as well as other parts of the Middle East on business or vacation.
