Case Vignette 37
A middle-aged man underwent non-myeloablative allogeneic hematopoietic stem cell transplantation for acute myeloid leukemia, receiving alemtuzumab just prior to the transplant. Recovery during the immediate post-transplantation period was unremarkable, but he remained on tacrolimus, mycophenolate and low-dose prednisolone for chronic graft-versus-host disease involving the skin, gastrointestinal tract and oral/conjunctival mucosa. Routine cytomegalovirus (CMV) screening of the blood was positive 2 months after the transplant, and oral valganciclovir was started. However, CMV viraemia was constantly detected thereafter (Figure 1), generally ranging between tens of thousands of copies per ml of blood for the most part, although there was never an evidence of CMV disease.
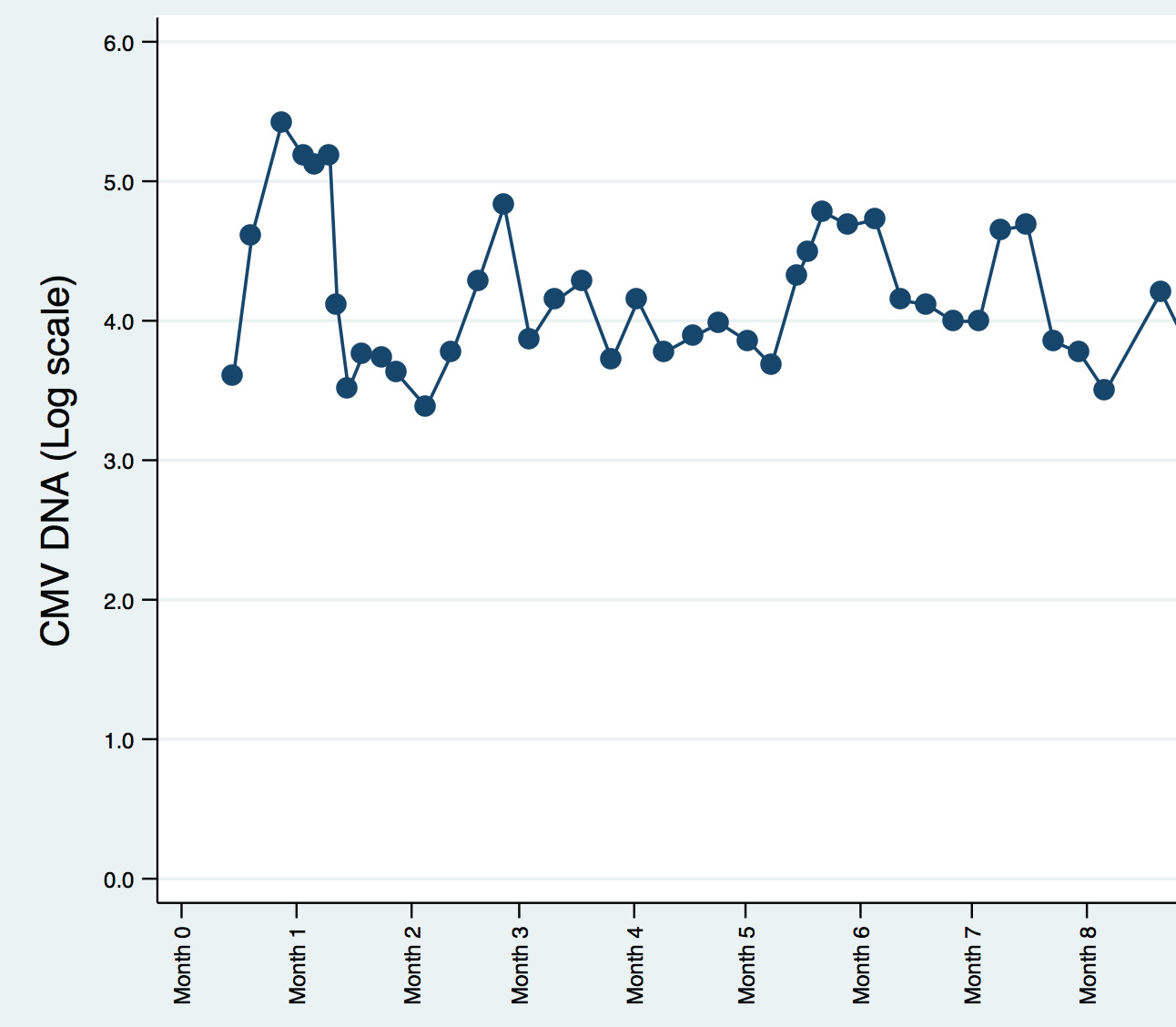
Cytomegalovirus (CMV) viraemia as determined by quantitative (in-house) CMV PCR over a period of 8 months.
Question: How should the CMV viraemia be managed?
[Updated 27th June 2015]
CMV viraemia – if detected earlier enough – represents CMV reactivation in most immunocompromised patients, and is often a precursor to CMV disease (i.e. if one or more organs are actually affected and damaged by the virus) rather than a manifestation of CMV disease itself. Treating CMV viraemia is considered “preemptive treatment” (i.e. treatment to “prevent disease”), rather than prophylaxis (starting antiviral treatment before either CMV viraemia or disease occurs) – the terminology can be somewhat confusing.
Alemtuzumab or campath is a monoclonal antibody targeting CD52 that has a profound and prolonged T-cell immunosuppressive effect, adding significantly to the already potent immunosuppressive effect of an allogeneic stem cell transplant. A “CMV management plan” is a must for patients treated with alemtuzumab, and there is a colourful and informative poster here by Bayer – the manufacturer of alemtuzumab, as well as an informative slide deck from the European Conference for Infections in Leukaemia (ECIL) in 2009 here. Nonetheless, both poster and slide deck fail to capture the great difficulty of managing some of these patients who have received alemtuzumab for allogeneic stem cell transplantation, and the patient described above is typical of such patients – with persistent viraemia despite multiple lines of therapy. The general principles of therapy still hold true, namely:
- Regular (twice-weekly) monitoring of CMV levels in blood, including checking for emergence of antiviral resistance if the patient is on ganciclovir or foscarnet for a prolonged period without evidence of viral suppression.
- Reduction of immunosuppressive therapy as far as possible (an infectious diseases physician will have to work in close coordination with the stem cell transplanter).
- Close monitoring of the patient for signs and symptoms suggesting development of CMV disease.
- Antiviral therapy – here, there is little good evidence, but many in clinical practice have tried combination antiviral therapy (i.e. ganciclovir and foscarnet), experimental therapy (i.e. artesunate) and adjunctive therapy (i.e. CMV immune globulins or IVIg).
There is no clear cut or “best practice” for such cases, as far as I know.
