Clinical Vignette 38
A young local man in his late 20’s, previously well, was found on pre-employment screening to have abnormal chest X-ray. He was otherwise asymptomatic.
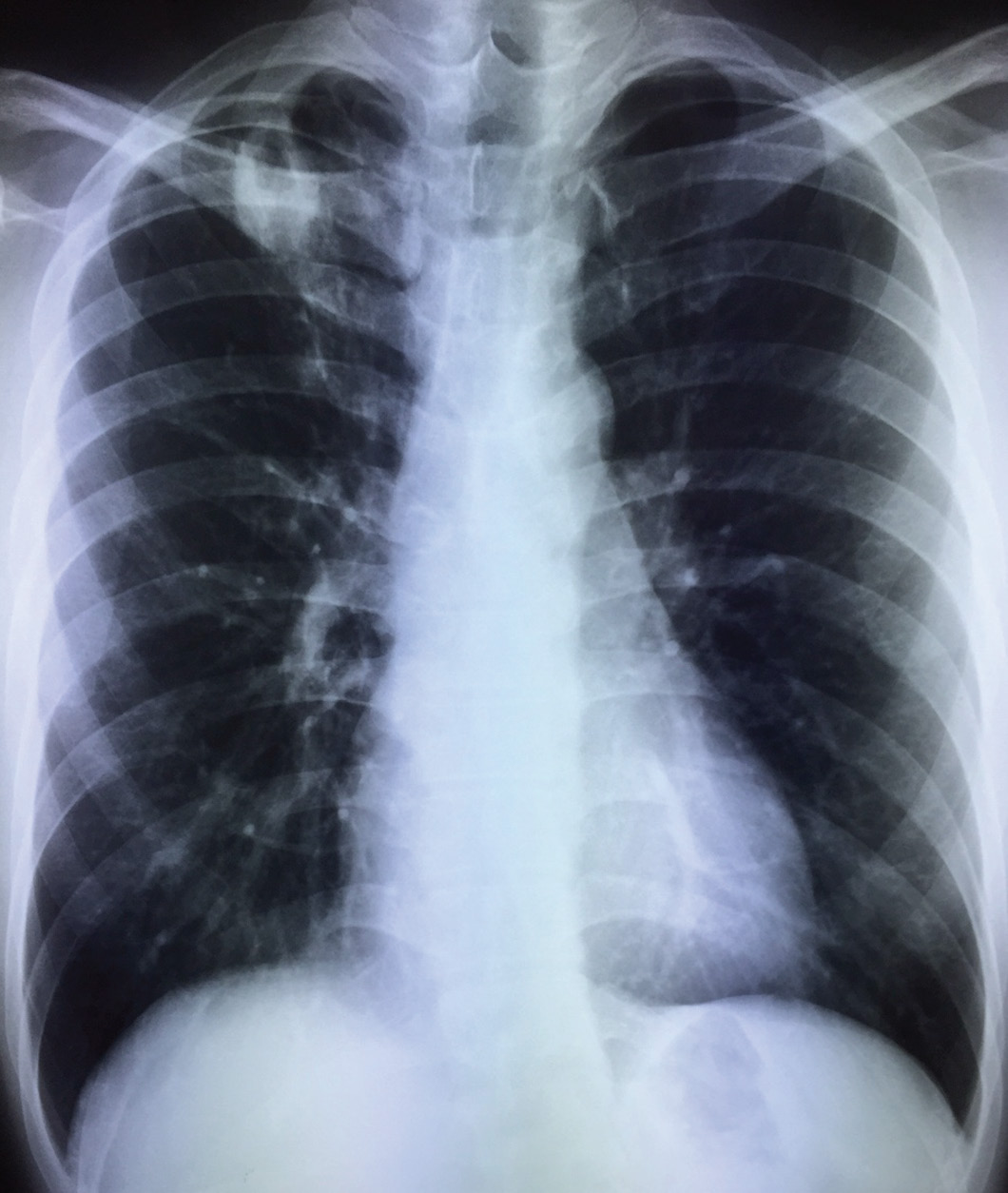
Chest X-ray of a young man, asymptomatic.
He underwent sputum induction for tuberculosis work-up (sputum microscopy and cultures for acid-fast bacilli, and PCR for Mycobacterium tuberculosis complex), and both sputum samples were negative for acid-fast bacilli on microscopy and MTC on PCR. A Mantoux test (or tuberculin sensitivity test) showed a reaction of 12 mm.
He had started to develop a dry cough a week later, although he did not have any fever or other constitutional symptoms. A repeat chest X-ray showed progression of radiological changes.

Chest X-ray of the young man, one week later.
However, repeat induced sputum for microscopy and MTC PCR did not yield any positive results, and sputum Gram-stain with bacterial cultures were also negative.
Question: How should one proceed – further investigations or empirical anti-tuberculous therapy?
[Updated 4 July 2015]
The most likely diagnosis remains pulmonary tuberculosis despite the negative sputum smears and TB PCR, because of the radiological appearance, the lack of any major immunosuppressive condition, and the relatively high rates of tuberculosis locally. He is also not in the age group where cancer is likely. The conundrum is whether to further investigate or start therapy. “Watchful waiting” is not a good option as there has been obvious radiological progression. The issue with further investigation is that a more invasive procedure, such as bronchoscopy with bronchoalveolar lavage and possibly transbronchial lung biopsy, will be necessary, with its attendant risks. A CT thorax is unlikely to yield more information that will impact on a therapeutic decision. The issue with empirical TB therapy is, naturally, what if this is not TB?
In any case, the pros and cons of each choice was discussed with the patient and empirical TB therapy was initiated. He tolerated the drugs well, cough resolved after a week, and follow-up chest X-rays showed progressive improvement as well. A significant minority of pulmonary TB cases in Singapore are culture negative.
