Clinical Vignette 51
A late middle-aged man presented with high fever for a day. He had been hospitalized for acute gastroenteritis a week ago, receiving intravenous fluids and oral fluoroquinolones. Clinical examination was unremarkable except for erythema around the previous IV plug site – there were no cardiac murmurs and lung auscultation revealed normal breath sounds.
He was prescribed IV ceftriaxone but fever persisted. A day later, his blood cultures flagged positive for MRSA and he was switched to IV daptomycin. A transthoracic 2D-echo showed a normal heart with no evidence of endocarditis. His fever subsided after 2 days of daptomycin and he felt subjectively better. However, on the third day of daptomycin therapy, he experienced right chest wall pain and slight breathlessness on walking to the bathroom. This failed to resolve with symptomatic treatment and chest X-rays were ordered.

Chest X-ray, PA view, of the patient with right-sided chest pain
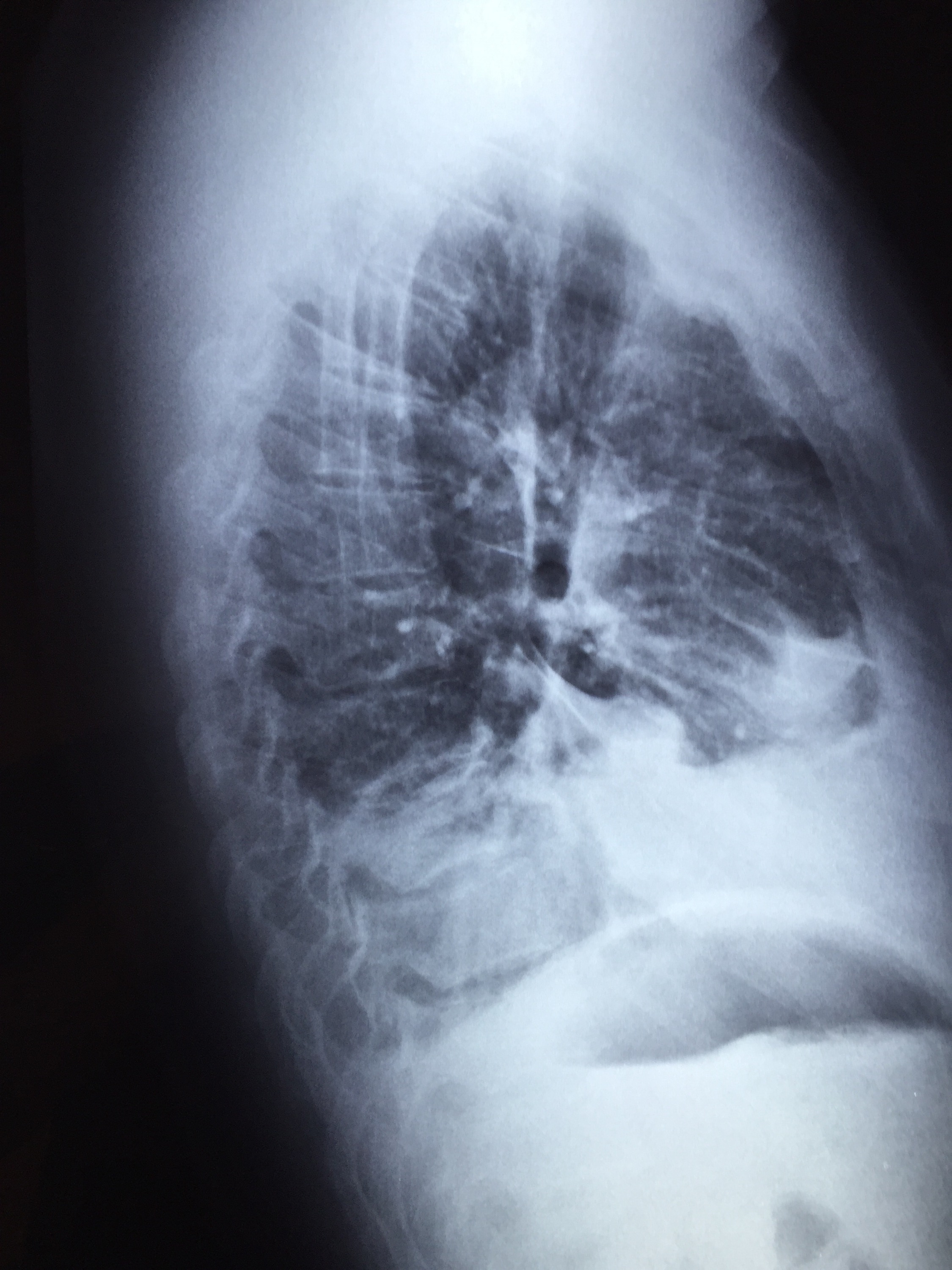
Chest X-ray of the same patient, right lateral view
Question: What is the likely diagnosis and how should the patient be managed?
[Updated 6 Jan 2016]
One of daptomycin’s unique and less desirable features is that the drug is broken down by lung surfactant, and hence it is inadequate for the treatment of pneumonia. In this particular case, the most likely scenario is a subclinical MRSA pneumonia that worsened even as the patient responded systematically to daptomycin, resulting in clinical pneumonia with parapneumonic effusion (an empyema cannot be completely ruled out at this stage as well, but is unlikely as daptomycin penetrates the pleura in adequate concentrations). He was switched to oral linezolid and recovered without any issues.
The question is, should all patients with systemic MRSA infection receive a chest X-ray prior to initiating daptomycin therapy? The answer seems to be “yes” at this stage, given the ease of availability and relative low cost of the chest X-ray.
