Broadly defined, healthcare-associated infections (HAIs, also termed “hospital-acquired infections” or “nosocomial infections”) are infections that occur during the process of care in a healthcare facility, most commonly a hospital. They are an important quality indicator for healthcare institutions – conceptually, one would not really wish to be treated at a hospital where one’s risk of acquiring an infection is high, in the same way one would try to avoid eating at restaurants with a high rate of gastroenteritis outbreaks. There is an important caveat here – HAI rates will vary according to the case mix of the hospital. A healthcare institution that handles more complex (i.e. more ill) cases and a higher proportion of emergencies will have a higher rate of HAI compared to one that primarily deals with obstetrics or elective orthopaedic operations, for example. Therefore one has to be careful making any inter-hospital comparisons.
It also turns out that for a significant proportion of infections in healthcare settings, it is challenging to tease out whether these infections originated from the community or from the hospital. Hence there are complicated definitions used in practice, such as the guidelines put up by the U.S. National Healthcare Safety Network (NHSN) and the European CDC. Because they are not easily classified, it is costly (in terms of time and trained manpower) to perform continuous surveillance of HAIs – there are no hospitals in Singapore that track the full “suite” of HAIs, for instance.
An alternative (and complementary in many respects) to continuous surveillance for HAIs that has become increasingly popular is to perform HAI “point prevalence surveys” (HAI-PPS). This is obviously not as robust as continuous surveillance, but is far less resource intensive, and offers “snapshots” of the situation that can be compared over time. This approach has primarily been championed in Europe, and you can find EU country-level results online, along with nice charts and tables showing the distribution of antibiotic use and antimicrobial resistance by country. The U.K. (now exiting the EU) also performs HAI-PPS – the protocol and forms used are virtually identical to the EU’s, and are available online. The results of their most recent survey are not yet available (done last year), but the earlier survey results have been published.
Our Ministry of Health funded the first local HAI-PPS as a research study in 2015 via the now defunct Communicable Diseases Public Health Research Grant (CD-PHRG). Led by Dr Kalisvar Marimuthu from Tan Tock Seng Hospital, this study scored several firsts: not only was it the first HAI-PPS conducted in Singapore, but it also involved virtually all public and private acute care hospitals in Singapore (except for Sengkang General Hospital and Farrer Park Hospital – then just being set up, the Institute of Mental Health, and Parkway East Hospital). This kind of large-scale collaboration between the public and private healthcare sectors in Singapore is virtually unprecedented, especially for research, and kudos to the senior management of the private (and public) hospitals for supporting the research team and ensuring that the work proceeded smoothly. On a more technical note, the European methodology and definitions were used whereas previously the majority of public sector infection control specialists preferred the American definitions by NHSN. This was primarily because the local results could then be compared to an international standard (in this case the Europeans) – the Americans have not performed point prevalence surveys on a country-wide scale.
The results of the initial survey, just published in Clinical Infectious Diseases (behind a paywall), were largely unsurprising. Of the 5,415 inpatients surveyed across 13 hospitals:
- HAI rates were high in local hospitals – 11.9% of inpatients were found to have HAIs.
- This is far higher than most European countries (EU HAI rate of 6%; country range 2% to 11%), but is possibly an issue of case-mix.
- Systemic (i.e. intravenous or oral) antimicrobial use was astoundingly high – fully half of the patients were on antibiotics and/or antifungals.
- To be more precise, 2,762 (51%) inpatients were prescribed 3,611 antimicrobial agents at the time of survey.
- Antimicrobial resistance rates were very high among the bacteria causing HAIs:
- 58% of all Staphylococcus aureus were methicillin-resistant (MRSA).
- 71.9% of all Acinetobacter spp. were resistant to the carbapenems.
- 37.7% of all Enterobacteriaceae were resistant to 3rd generation cephalosporins, while 7% were resistant to the carbapenems.
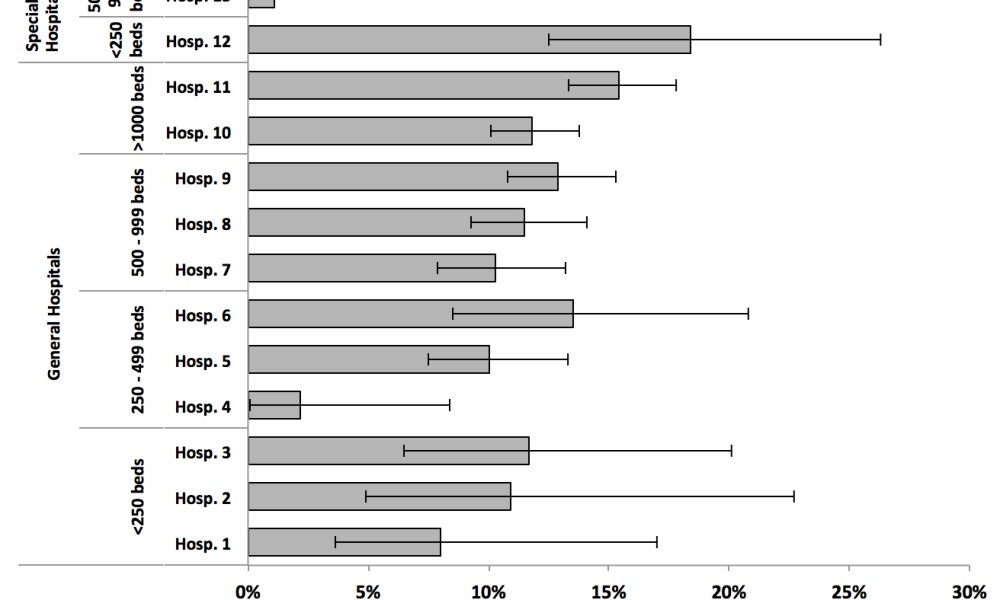
Individual hospital results for HAI prevalence are available in the supplemental appendix (also behind a paywall) as a chart, reproduced below.
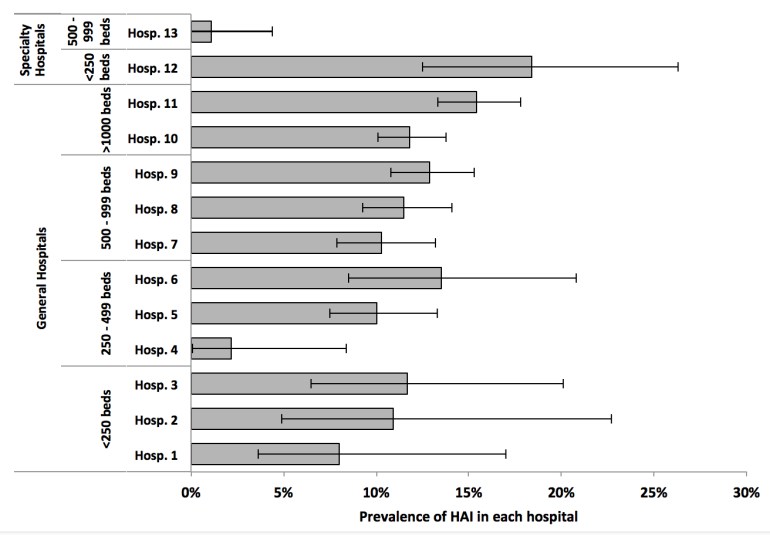
Supplemental Figure 2 from the Singapore HAI-PPS study published in Clinical Infectious Diseases.
How do the private sector hospitals compare with the public sector hospitals? This result is not available in the publication but the research team kindly allowed it to be published in last year’s edition of Parkway’s “Reflections on Quality” periodical, which is unfortunately not available online. A far higher proportion of inpatients (exceeding 65%) at private sector hospitals were on systemic antimicrobial agents at the time of survey compared to inpatients at public sector hospitals – close to 7% were on 3 or more antimicrobial agents whereas this figure was <3% in inpatients at public sector hospitals. However, the HAI rates were equivalent in acute hospitals from both sectors.
This work has been a resounding success (my view potentially biased by being part of the study team and a co-author on the paper) and has brought up many interesting questions that should be investigated in further studies: for example, far more patients are on antibiotics than there are infections, even taking into account those infections that originated from the community. Even more importantly, follow-up HAI-PPS should be performed to track how our hospitals have performed in containing HAIs. Surveys like these, performed by independent auditors, and with a methodology agreed upon by all participating institutions, are less susceptible to perceptions of biased reporting and data manipulation.

Impressive..!Thanks for the post..
LikeLiked by 1 person