Clinical Vignette 31
A middle-aged man with well-controlled diabetes mellitus was diagnosed with acute promyelocytic leukaemia (APML). He completed both induction and consolidation with all-trans retinoic acid (ATRA) and idarubicin, and was in remission. He was subsequently maintained on outpatient weekly low-dose methotrexate (25 mg/week) and 6-mercaptopurine. Six months later, he presented with fever and cough for 2 weeks, with whitish phlegm produced on coughing. There was mild exertional dyspnoea but no other symptoms such as chills, night sweats, weight loss, or appetite loss. There was no significant contact or travel history.
Clinical examination was unremarkable except for a drop in SpO2 to 92% after a brisk walk around the hospital room. The chest X-ray showed faint miliary shadows in both lung fields (the CXR image is provided below, but unfortunately the resolution is insufficient to permit visualisation of the abnormalities), which was confirmed on CT thorax.
Chest X-ray of the middle-aged man with fever and cough for 2 weeks.
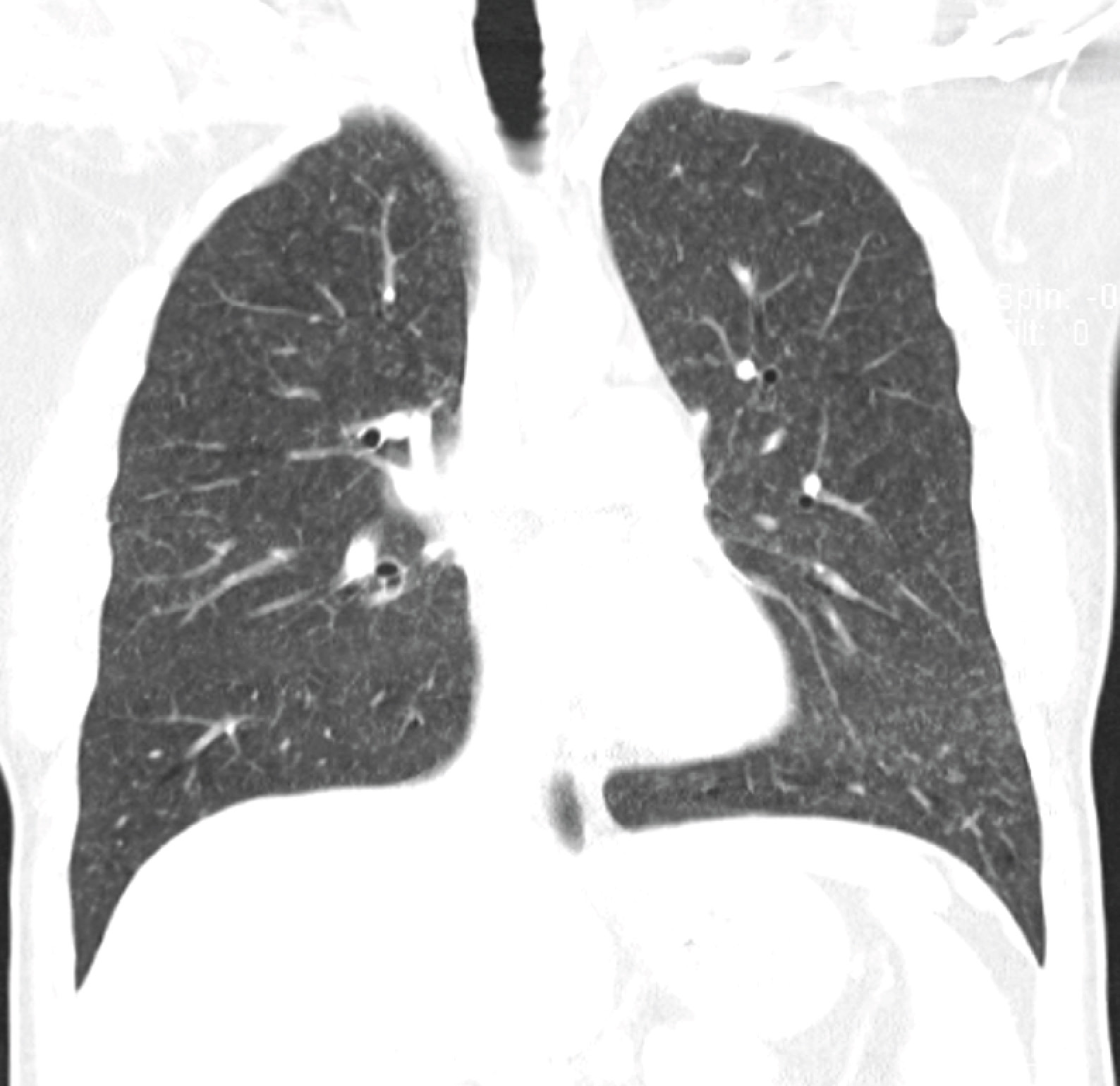
CT thorax (lung window) showing very small nodular shadows in both lung fields (coronal cut).

CT thorax (lung window) showing very small nodular shadows in both lung fields (transverse cut).
Question: What are the major differentials and what do you think is the diagnosis here?
[Updated 9th May 2015]
There are a few infectious diseases that may present similarly, including miliary tuberculosis, Pneumocystis jiroveci pneumonia (PCP) and viral (mainly herpesviruses in view of fairly prolonged symptoms) pneumonitis. Both PCP and viral pneumonitis would be unusual in such a host, where the immunosuppression is not profound. Miliary tuberculosis is possible, but hypoxia is unusual at the stage where the patient is still relatively well.
The major non-infectious differential is methotrexate pneumonitis. The best review on this topic (in my opinion) was written 15 years ago – a large case series and literature review published in the European Respiratory Journal. The symptoms and clinical presentation are consistent, and nodular infiltrates alone are seen in 4.1% of cases. It is also interesting to note that granulomas are a common histological finding.
For this patient, we stopped the weekly chemotherapy (he was in any case in remission) and his symptoms resolved within a couple of weeks.
