Clinical Vignette 47
A teenaged girl presented with high fever (up to 40 degrees Celsius), headache, and a dry cough for 4 days. She did not have prior symptoms of an upper respiratory tract infection such as sore throat or runny nose. None of her friends or family members were recently ill, and she has not traveled out of the country for a couple of years.
On clinical examination, there were coarse crackles over the right lower lung field. Her oxygen saturation was 95% on room air. Her blood pressure was 91/54 mmHg. There were no cardiac murmurs audible nor a rash. Her white cell count as elevated (14K), with predominantly neutrophils. Renal function was normal and the chest X-ray is shown below.
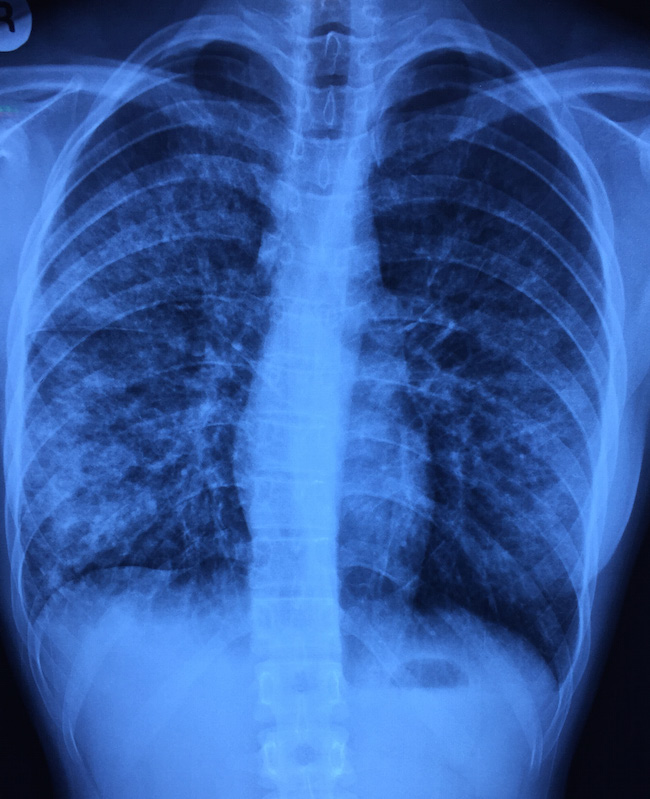
Chest X-ray of the teenager with acute onset of fever and cough.
Questions: What is the diagnosis and the likely aetiology? How should this young girl be managed?
[Updated 10 Oct 2015]
The chest X-ray shows bilateral infiltrates, far more prominent on the right where the abnormal breath sounds were heard. The appearance is not that of a dense lobar consolidation that is more associated with pneumococcal pneumonia. Some posters on Facebook have suggested Pneumocystis jiroveci pneumonia (PCP or PJP) if the setting is right. She did have one sexual partner, but only for one year (having said which, such history is often unreliable), and the progression is much too fast for PCP in a patient with HIV.
A HIV test was performed nonetheless (negative), and she was started on antibiotics as for community-associated pneumonia (ceftriaxone and clarithromycin, given the appearance of the X-ray). However, all bacterial cultures from blood and sputum were negative, and a throat swab came back positive for influenza A. Multiple studies, including this recent one from NEJM, have shown that respiratory viruses as a group are the most common cause of community-associated pneumonia, even those requiring hospital admission. It is important to consider this possibility and order the appropriate tests (which unfortunately are more expensive than a course of subsidised antibiotics in our public sector hospital setting!) in order not to over-treat the patients with more broad-spectrum antibiotics when symptoms fail to resolve with initial antibiotics.
This teenager made a complete recovery with supportive care. She did not receive oseltamivir or other neuraminidase inhibitor therapy.
