Clinical Vignette 8
A middle-aged man presented with a low-grade fever (37.8 degrees Celsius) and sudden pain over his right thigh for 3 days, which did not resolve with painkillers. He has a history of diabetes mellitus, and had a road traffic accident 30 years ago resulting in the fracture of his right femur. This was repaired (open reduction and internal fixation) without the use of any implants at that time, and had not caused any trouble since.
Clinical examination revealed mild erythema over the anterior surface of his right thigh. The X-ray is shown below.
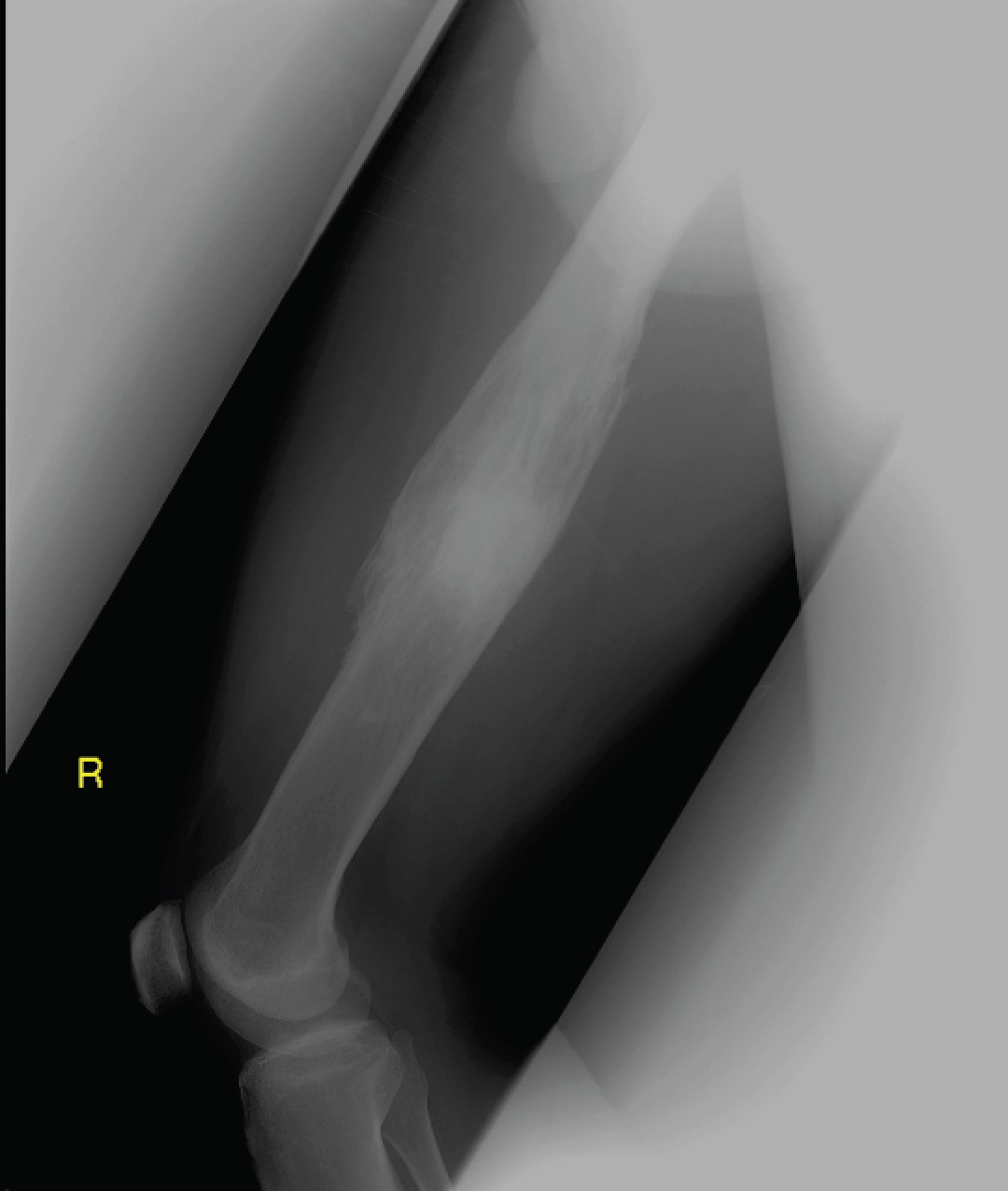
X-ray of the right femur.
Question: What is the diagnosis and what confirmatory tests should be performed?
[Updated 22nd November 2014]
This gentleman has chronic osteomyelitis of the femur resulting in mal-union and a central sequestrum (dead infected bone) with surrounding involucrum (new bone growth as a result of infection). These features are better appreciated on magnetic resonance imaging (MRI) – and a sample image is shown below.
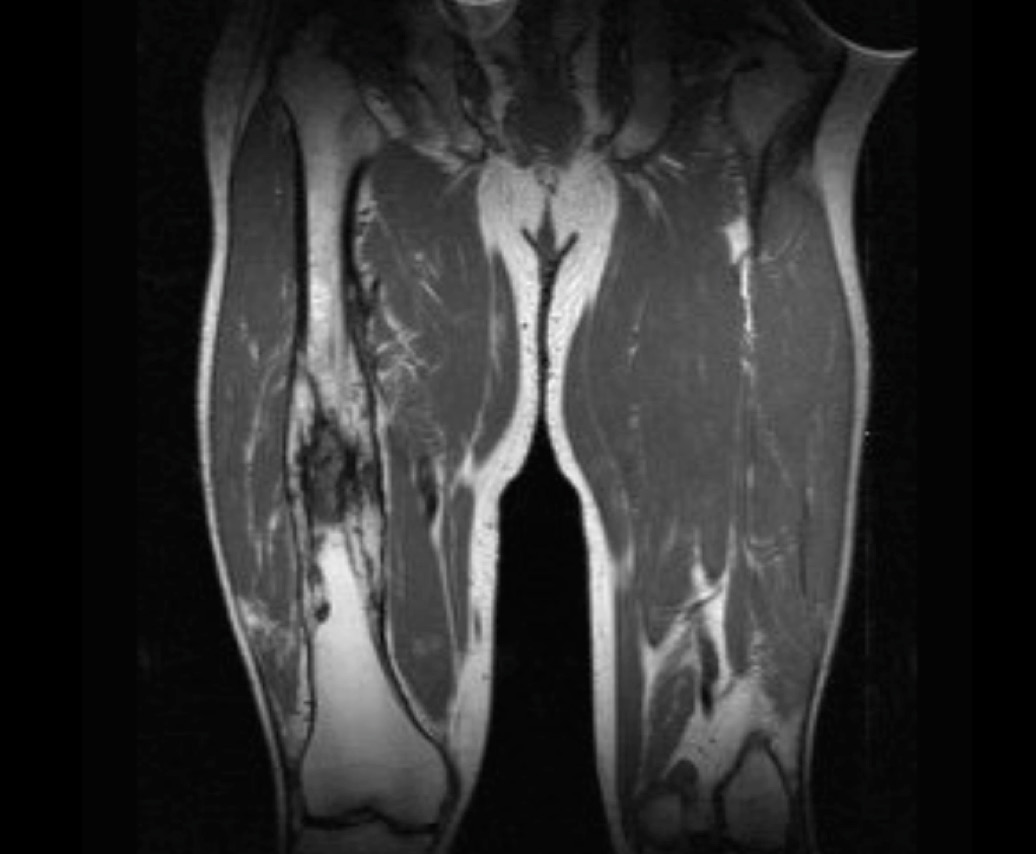
MRI of the femur showing (on the right femur) the changes of chronic osteomyelitis.
Chronic osteomyelitis is a surgical condition, and ideally all the dead and infected bone should be debrided and removed, because antibiotic penetration into dead bone is very poor, and antibiotic therapy alone – even if given for a very prolonged duration – may result in treatment failure and relapse in up to 20+% of such cases. The other reason for surgical intervention is to obtain a microbiological diagnosis. Cultures from other sites (i.e. blood) tend to be negative.
This gentleman had MRSA growing from intra-operative bone cultures. It is likely that the organism had been there since 30 years ago, gradually causing a worsening infection. He received 6 weeks of intravenous antibiotics (after extensive debridement and washout of the infected site), and recovered fully.
