Clinical Vignette 40
A healthy man in his late middle age presented with sudden onset of fever. This was associated with back and muscle ache, as well as mild lower limb weakness and lethargy. He saw a general practitioner and obtained relief from his symptoms with the prescription of antipyretics (including a shot of NSAIDs). However, his muscle aches persisted, and he developed neck and headache on the third day of illness. By the 5th day of illness, he was noted to have an unsteady gait, with headache, nausea and vomiting. He was then hospitalised, where on physical examination, he was found to have neck stiffness, a fever of 38.6 degrees Celsius, and left-sided hemiparesis. There was no recent travel or contact history of note, nor had he been abusing any drugs/medications.
He was treated with high dose intravenous (IV) ceftriaxone and IV ampicillin, as well as IV dexamethasone for presumptive meningitis +/- brain abscess. The relevant MRI images done on the same day are shown below:
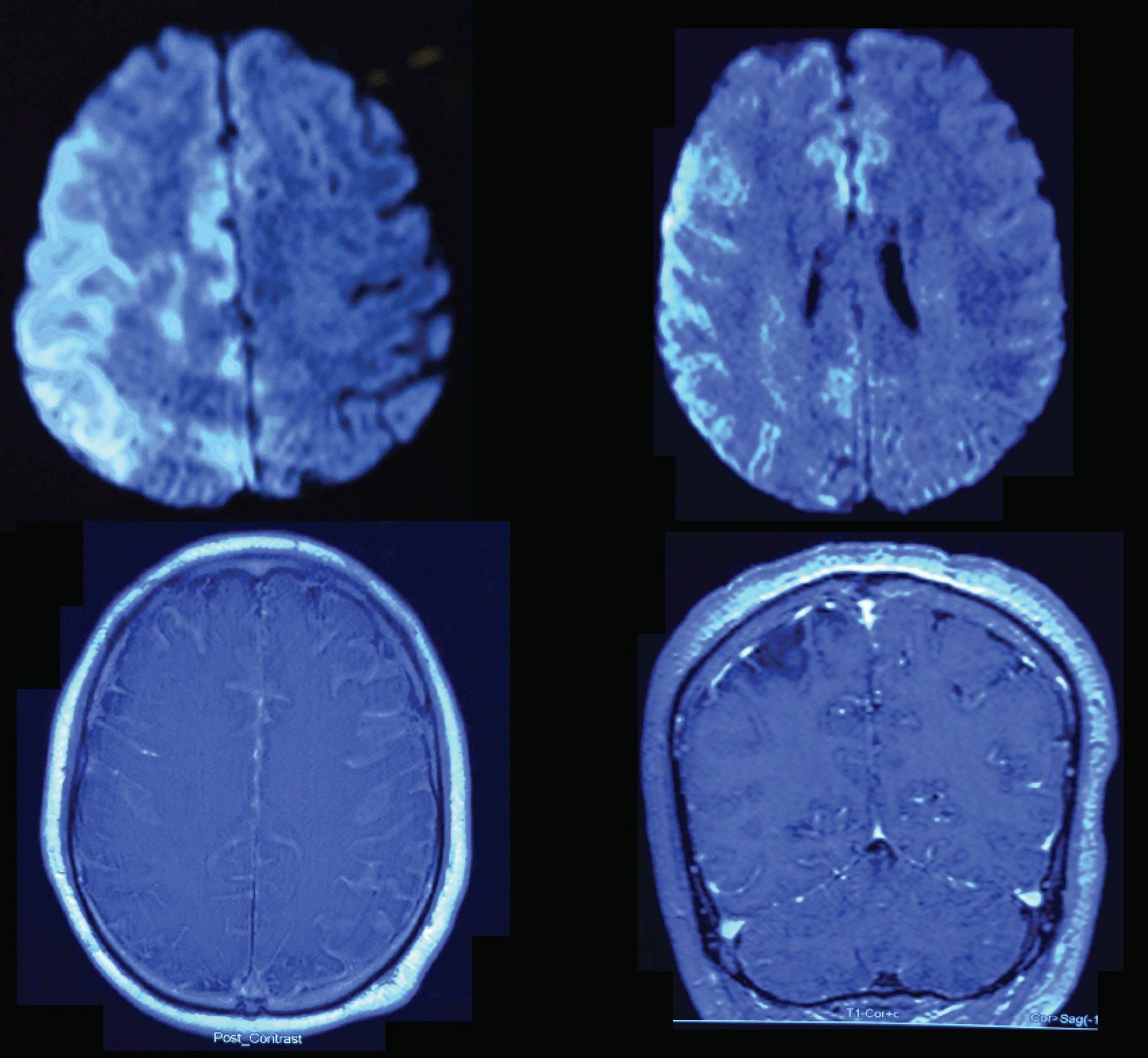
MRI images of the man with fever and left hemiparesis.
That night, his weakness progressed to become complete left hemiplegia, and he became drowsy, requiring intubation with medical ventilation in the intensive care unit for airway protection. The next day (within 12 hours), his blood cultures flagged positive, with Gram-positive cocci seen on Gram stain.
Question: What is the likely organism causing his illness?
[Updated 8 August 2015]
In the context of the recent Group B Streptococcus outbreak, the answer is Streptococcus agalactiae. Note that this would have been the wrong choice in any other scenario, as the most likely organism is Streptococcus pneumoniae.
Unfortunately, the patient passed away within 72 hours despite maximal medical care.

Streptococcus pneumoniae.
Should add IV Vancomycin for penicillin-resistant pneumococci?
LikeLike
[…] The outbreak is technically over, but the publications are starting to appear. Here is a local work describing a subset of 14 patients with GBS brain infections, showing a unique pattern of imaging appearances, just published in the Journal of Magnetic Resonance Imaging (alas behind a paywall). I had previously shown the MRI images of a man with ST283 GBS meningo-encephalitis as a clinical vignette. […]
LikeLike