
Clinical Vignette 82
A final clinical vignette (for a while, at any rate) before more substantive posts.
A middle-aged man with a decades-long history of bronchiectasis presented with worsening cough with productive sputum, decreasing effort tolerance, low grade fever, and weight loss over 2 months. He has no other co-morbid conditions.
Chest X-ray showed worsening bilateral infiltrates – particularly on the right – and two courses of oral antibiotics (augmentin first followed by ciprofloxacin) produced only transient relief.

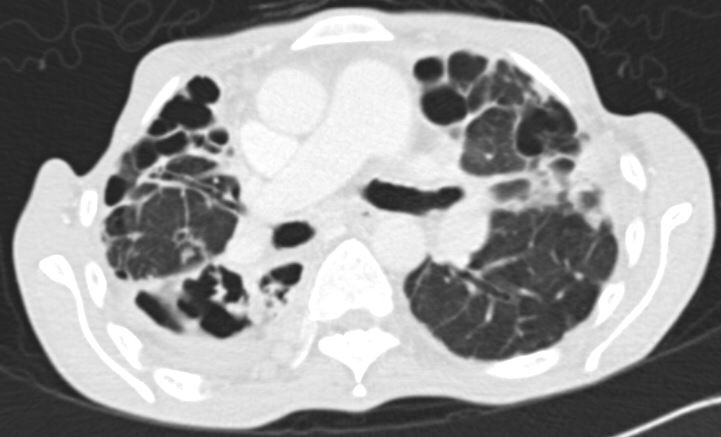
Sputum sent for acid-fast bacilli (AFB) smear was positive, and mycobacterial cultures were positive in two weeks for Mycobacterium abscessus. A repeat sputum sample yielded the same result. A CT thorax was performed, showing essentially worsening of bronchiectasis.
Question:
- How would one manage this man?
[Updated 11 March 2018]
This patient fulfils criteria for M. abscessus pulmonary disease, although it can be technically challenging to decide if deterioration of pulmonary function is due to the infection or to other factors influencing bronchiectasis.
The British guidelines for managing non-tuberculous mycobacteria-associated pulmonary disease can be found here, just updated last year. It is remarkable how little high quality evidence there exists today
The American Thoracic Society/Infectious Diseasea Society of America guidelines are being updated at this point (previous version was 2007, reflecting perhaps a relatively neglected disease).
In addition to optimising treatment for bronchiectasis, the British Thoracic Society experts recommend an initial phase (at least 4 weeks) with oral clarithromycin or azithromycin if the organism is not resistant to macrolides, along with intravenous amikacin, tigecycline and imipenem. The continuation phase includes nebulised amikacin with 2-4 antibiotics depending on drug susceptibility testing: a macrolide, clofazimine, linezolid, a tetracycline (doxycycline or minocycline), a fluoroquinolone, and/or cotrimoxazole.
In Singapore, intravenous cefoxitin is commonly prescribed during the intensive phase, but use of nebulised amikacin is rare.
Surgery is an option for patients with localised disease, but that is not the case for the patient in this particular clinical vignette.
